





Abstract
Unexpected azygos vein injury during thoracoscopic lung resection is rare. Here, we describe a case of azygos vein arch injury caused by an ultrasonic scalpel. The patient underwent segmentectomy for right upper lobe lung cancer. The ultrasonic scalpel was activated while its blade tip was inadvertently grasping the vascular wall of the azygos vein arch during management of bleeding from the pulmonary artery stump, resulting in injury to the azygos vein arch. Because the injury site was temporarily sealed, it was not initially detected. When the right upper lobe was retracted ventrally to dissect the upper lobe bronchus, tension was applied to the injured site of the azygos vein arch, leading to massive haemorrhage. Conversion to thoracotomy was required, and haemostasis was achieved using a fibrin sealant patch. The azygos vein is a low-pressure system; most injuries can be managed with a fibrin sealant patch.
Introduction
The reported frequency of unexpected intraoperative vascular injury during anatomical lung resection via video-assisted thoracoscopic surgery (VATS) is 2.9%–6.3% [1–3]. Pulmonary artery injuries are the most common (71.6%–80.8%), whereas azygos vein injuries are rare (3.0%–7.7%) [2, 3]. Accordingly, there are few detailed reports of azygos vein arch injury [3–7]. Additionally, 34.6%–37.3% of vascular injuries occur during the use of energy devices, such as ultrasonic scalpel (US) or advanced bipolar device [2, 3], often resulting from technical or visual insufficiency [8]. Herein, we report a case of secondary azygos vein arch injury caused by the use of a US under poor surgical visibility during persistent bleeding from the pulmonary artery stump.
Case report
A 69-year-old woman with dyslipidaemia and a history of breast cancer surgery underwent computed tomography, which revealed right upper lobe lung cancer (T1miN0M0, stage IA1) (Fig. 1A). She had a 3 pack-year smoking history, and spirometry findings were within normal limits. She was not receiving anticoagulant therapy. A right S2 + S3a segmentectomy via hybrid VATS was planned (Fig. 1B and C) [9]. Intraoperatively, the ascending A2 was divided, and bleeding was observed from its distal stump. While preparing soft coagulation for haemostasis, the bleeding point was compressed using a surgical cotton swab, and the interlobar fissure between the upper and lower lobes was separated using a US (Fig. 2A). The US was activated while its blade tip was inadvertently grasping the vascular wall of the azygos vein arch, resulting in injury to the azygos vein arch. At that time, the injury site was sealed, and the injury was not detected. Bleeding from the distal stump of ascending A2 was controlled using soft coagulation (Fig. 2B). When the right upper lobe was retracted ventrally to dissect the upper lobe bronchus, tension was applied to the injured site of the azygos vein arch, and a 5-mm-diameter hole was identified at the origin of the azygos vein arch (Fig. 2C and D). Massive haemorrhage occurred, and blood pressure decreased from 70/40 to 50/30 mmHg. Rapid intravenous infusion of hydroxyethyl starch and compression of the bleeding site using the adjacent lung resulted in recovery of blood pressure. Conversion to thoracotomy was required. The proximal side of the azygos vein arch was secured. Although it was necessary to secure the main trunk of the azygos vein and multiple intercostal veins on the distal side, doing so while compressing the bleeding point was challenging. Therefore, a fibrin sealant patch (TachoSil®; Corza Health, San Diego, CA, USA) was applied to the mediastinum, including the injury site of the azygos vein arch, and haemostasis was achieved (Fig. 2E). The segmentectomy was subsequently completed as planned (Fig. 2F). The operation time was 237 min, and the amount of blood loss was 1070 mL. No blood transfusion was required during the perioperative period. Postoperatively, no intrathoracic haematoma was observed on chest radiography (Fig. 3). The chest tube was removed on postoperative day (POD) 2, and the patient was discharged on POD 6. The surgical scheme is shown in Fig. 4, and the surgical video is provided in Video 1. No recurrence of lung cancer was observed at the 1-year follow-up.
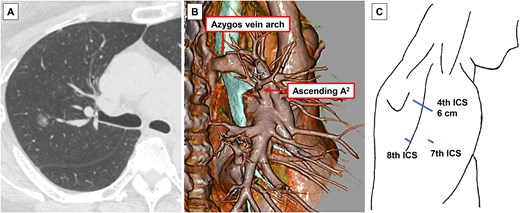
Preoperative imaging findings and surgical incision. (A) Computed tomography (CT) showing a 1.2-cm radiological part-solid lung nodule in the right upper lobe. (B) Three-dimensional CT imaging. (C) Surgical incision. ICS, intercostal space.
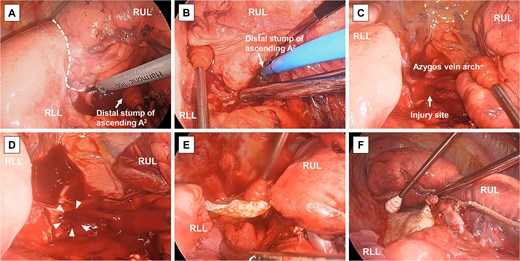
Surgical findings. (A) The interlobar fissure between the right upper lobe (RUL) and right lower lobe (RLL) (dotted line) is separated using an ultrasonic scalpel while compressing the bleeding point at the distal stump of the ascending A2. (B) Bleeding from the distal stump of the ascending A2 is controlled using soft coagulation. (C) The injury site of the azygos vein arch is temporarily sealed. (D) A 5-mm-diameter hole (white arrowheads) is observed at the injury site following mobilisation of the RUL, resulting in massive haemorrhage. (E) A fibrin sealant patch is applied to the injury site. (F) The surgical field after right S2 + S3a segmentectomy.

Postoperative chest radiography. A chest drain tube is placed in the right thoracic cavity, and no intrathoracic haematoma is observed.
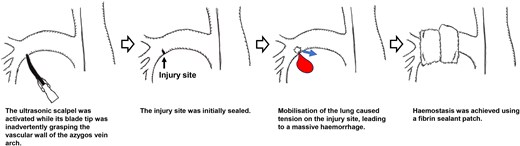
Surgical schema.
Informed consent was obtained from the patient for publication of this case report, which was approved by the Institutional Review Board of our institution (25-97; 19 December 2025).
Discussion
The main patterns of vascular injury caused by a US include puncture injury by the blade (known as ‘drilling’) and thermal injury from the heated blade [2, 3]; however, the injury pattern in this case differed from both. In this case, activation of the US while the blade tip was inadvertently grasping the vessel wall resulted in injury to the azygos vein arch. Although the injury site was temporarily sealed, subsequent mobilisation of the lung caused tension at the site, leading to bleeding. Considering these potential risks, the US should be used while constantly confirming the position of the blade tip and ensuring that surrounding tissues are not inadvertently grasped. In this case, bleeding from the pulmonary artery stump resulted in poor surgical visibility, leading to secondary injury of the azygos vein arch. Because secondary injury can be more fatal, if unexpected intraoperative bleeding occurs, it is crucial to achieve complete haemostasis before proceeding to the next surgical step.
Reported cases of azygos vein arch injury are summarised in Table 1 [3–7]. In approximately half of the cases, haemostasis was achieved by suturing the injury site. When attempting suture closure, it is desirable to secure the vessel on both sides of the injury. In the present case, the bleeding point was located at the origin of the azygos vein arch, and securing multiple distal vessels was challenging while compressing the injury site with a surgical cotton swab. Furthermore, the bleeding was too severe to permit suture closure without securing the azygos vein. The azygos vein arch drains into the superior vena cava, where the pressure is 8–12 mmHg [10]. In an in vitro haemodynamic study using a tubing system, a ≤ 10-mm-diameter hole sealed with TachoSil® withstood pressures up to ~60 mmHg [11]. Therefore, most cases of azygos vein arch injury, including the present case, can be managed with a TachoSil® patch. The choice of vascular repair should be determined not only by the location and size of the injury but also by whether the injured area can be adequately covered with a fibrin sealant patch and whether dead space remains around the injury site.
Reported cases of azygos vein arch injury during thoracoscopic lung cancer surgery.
| Author | Year | Surgical procedure | Situation of injury | Use of surgical device | Conversion to thoracotomy | Method of haemostasis |
|---|---|---|---|---|---|---|
| Flores RM et al. [4] | 2011 | RUL | Mediastinal nodal dissection | Unknown | Yes | Primary suture |
| Yamashita S et al. [3] | 2013 | Unknown | Unknown | Unknown | Yes | Primary suture |
| Liang C et al. [5] | 2013 | RUL | Dissection of hilum | Unknown | Yes | Cut of azygos vein arch |
| Xiao ZL et al. [6] | 2014 | Unknown | Dissection of hilum | Electrocautery hook | No | Primary suture |
| Fernández Prado R et al. [7] | 2014 | Unknown | Mediastinal nodal dissection | Electrocautery hook | No | Cut of azygos vein arch |
| Present case | 2026 | RUS | Separation of interlobar fissure | Ultrasonic scalpel | Yes | Fibrin sealant patch |
Abbreviations: RUL, right upper lobectomy; RUS, right upper segmentectomy.
The primary strength of this report lies in the rarity of azygos vein arch injury, coupled with the uncommon pattern of vascular injury caused by US. A major limitation is the limited number of similar reports on vascular injuries. Accumulation of additional case reports may contribute to improved surgical outcomes.
Acknowledgements
We would like to thank Editage (http://www.editage.jp) for assistance with English language editing.
Conflicts of interest
None declared.
Funding
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}