





Abstract
The use of reinforced linear stapling devices is standard during distal pancreatectomy. We report rare cases of reinforced linear staples falsely appearing on post-operative imaging as retained foreign bodies. Two patients underwent laparoscopic subtotal pancreatectomy with use of a reinforced linear stapling device. Cross-sectional imaging obtained in the post-operative period showed fluid collections containing what was described as a free-floating foreign body. One patient underwent reoperation due to the imaging findings. The reported foreign bodies in both patients were in fact the reinforced staple lines used to transect the pancreas. Understanding this phenomenon led to changes in management in both patients with less invasive treatment than would otherwise have been performed. Reinforced staple lines used during distal pancreatectomy can have a misleading appearance on post-operative imaging. An understanding of this possibility is important to avoid unnecessary invasive procedures.
Introduction
Postoperative pancreatic fistula is a known and dreaded complication of both subtotal and distal pancreatectomy. Transection of the pancreas is usually performed with linear staplers, and there is evidence to support staple-line reinforcement to decrease the incidence of fistulas [1, 2]. Surgical staple lines and reinforcement are known to be radio-opaque. They present characteristic findings that are usually easy to differentiate from unintentionally retained foreign bodies.
The failure to retrieve foreign bodies unintentionally left behind during surgery is a serious medical error. It can give rise to legal action, have medical complications, and cause significant psychological harm caused to the patient [3]. These mistakes are associated with high monetary costs, both medically and legally [3].
We report two cases in which the reinforced staple line was seen in post-operative imaging as a free-floating object within a small post-operative fluid collection, mistakenly identified as a retained foreign body. This case report is reported in line with the SCARE Criteria [4]. Informed consent was obtained from all participants. The participants were informed about the procedures involved, the possible risks and benefits, and their right to withdraw their consent at any time without repercussions. All collected information was treated with strict confidentiality and anonymity.
Case presentation
Case 1
The first patient is a 71-year-old male with significant past medical history of gout, gastroesophageal reflux disease, sleep apnea, obesity, and hyperlipidemia. He underwent subtotal pancreatectomy and splenectomy for a pancreatic duct associated with chronic pancreatitis. After adequate peripancreatic and retropancreatic dissection, the pancreas was transected with linear surgical stapler with staple line reinforcement. The splenic artery and vein were divided separately, and no drain was left in place. Final pathology showed undifferentiated anaplastic carcinoma with extensive fibrosis and sarcomatoid features, margins were free and zero lymph nodes out of 24 retrieved were positive for malignancy. Surgery was uneventful, and he was discharged on postoperative day (POD) 5.
The patient was readmitted several times for recurring episodes of pancreatitis, and follow-up imaging showed a fluid collection in the surgical bed, with a floating staple line inside (Fig. 1). The radiologist reported a retained foreign body. However, the surgeon suspected the radiographic findings to be the free-floating end of the staple line. After much discussion, the patient received supportive treatment for his pancreatitis but no direct treatment for the imaging findings of reported foreign body. He did not receive percutaneous drainage nor antibiotic treatment. After treatment of the patient’s pancreatitis, he did not have recurrent issues attributable to the imaging findings. He completed adjuvant chemotherapy and has been free of recurrent disease or other complications for over 3 years.

Postoperative CT demonstrating a small fluid collection in the pancreatic resection bed containing a radiopaque structure (reinforced staple line).
Case 2
The second patient is a 61-year-old female with a past medical history of chronic bronchitis, gastroesophageal reflux disease, diverticulitis, lymphadenopathy, mixed hyperlipidemia, and rheumatoid arthritis. She underwent a subtotal pancreatectomy for a pancreatic neuroendocrine tumor (NET) which had increased in size, from 12 mm to 18 mm in a span of 3 years. The pancreas was transected with a linear stapler also using staple line reinforcement. The vessels were transected separately. The specimen showed an intermediate grade neuroendocrine tumor, margins free, zero out of 51 lymph nodes involved by tumor. Surgery was uneventful and she was discharged on POD 3.
The patient was readmitted one month after, with nausea and vomiting, and was found to have a 6.6 cm fluid collection in the surgical bed. The radiologist described a foreign object, potentially a catheter fragment, detected within the collection (Fig. 2). Much discussion was had between the surgical team and multiple radiologists, who have extensive experience in evaluating cross-sectional imaging of the pancreas. The patient was taken back to the OR on the following day for a diagnostic laparoscopy. Findings included a thick capsule around the fluid collection with no free intra-abdominal communication. Intraoperative ultrasound was used to evaluate the contents of the fluid collection (Fig. 3). The acoustic shadow of the staples on the staple line along with its characteristic shape was identified. The staple line was seen to be partially detached from the pancreas and floating inside the fluid collection. To avoid disrupting the encapsulated fluid collection and possibly creating an uncontrolled fistula, the collection was not entered. Instead, a post-operative endoscopic cystogastrostomy was performed to drain the fluid. The staple line was clearly seen endoscopically during creation of the cystgastrostomy (Fig. 4), confirming there was no inadvertently retained foreign body. The patient’s symptoms resolved after the procedure, and she had no further complications.

CT in Case 2 showing a postoperative collection with an apparent free-floating radiopaque object within the cavity.
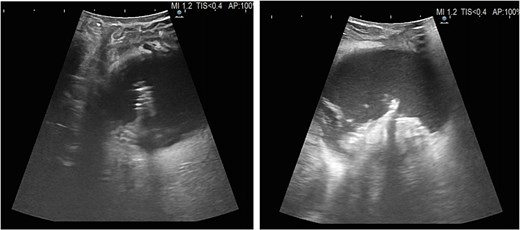
Intraoperative ultrasound demonstrating the characteristic acoustic shadow and shape of the staple line within the encapsulated collection.
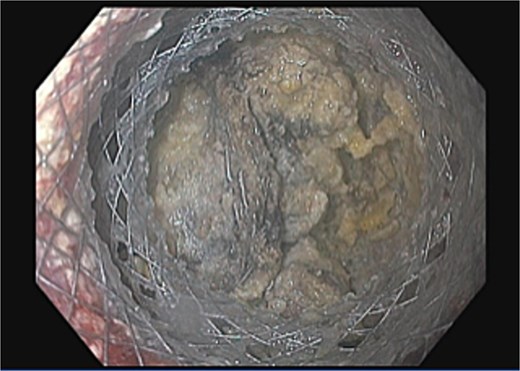
Endoscopic view during cystogastrostomy creation demonstrating the staple line within the collection, confirming expected surgical material.
Discussion
Imaging diagnosis is sometimes challenging, especially in patients with altered anatomy due to surgical intervention and surgical material. We present two unusual cases in which a detached staple line presented as a free-floating foreign body on imaging. The radiologists that reviewed the imaging have extensive experience with pancreatic imaging including in post-surgical patients but still were misled by the findings.
The partial separation of the staple line from the pancreas may be due to pancreatic fracture, which could lead to a pancreatic leak and explain the postoperative fluid collections. There may also be an element of pancreatic ischemia at the staple line contributing to the fracture. This would explain the appearance on imaging.
It is conceivable that the staple line reinforcement accentuated the abnormal appearance of the staple line to make it seem like a retained foreign body. It showed a serpiginous appearance that was maintained even after detachment from the pancreas, which is not a typical appearance of staple lines.
The misinterpretation of a staple line as an inadvertently retained foreign body places the surgeon and the patient in a difficult situation. Erroneous exploration to extract a misdiagnosed foreign body can lead to unnecessary increase in risk of morbidity. Knowledge about this potential finding on computed tomography (CT) is important to correctly weigh treatment options without subjecting the patient to unnecessary interventions.
We consider the present report to be important as it helps other surgeons make informed decisions regarding the most appropriate management approach for patients that have floating material inside a pancreatic fluid collection. Unfortunately, it can be difficult to differentiate between unwanted foreign bodies versus expected foreign bodies, such as surgical staple lines. Thus, individualized clinical and surgical decision making is important in each situation. These findings may contribute to the nuances of that decision making. Furthermore, they may aid in multidisciplinary discussion, which is crucial during treatment of pancreatic surgical patients.
Conclusions
Reinforced staple lines used during distal pancreatectomy can mimic retained foreign bodies on postoperative imaging. Awareness of this phenomenon may prevent unnecessary reoperations and guide safer patient management.
Conflicts of interest
The authors declare no conflicts of interest.
Funding
No funding was received for this study.
Consent for publication
Written informed consent was obtained from both patients for publication of this case report and accompanying images.

{kind=link}
{kind=link}
{kind=link}
{kind=link}