





Abstract
Eccrine porocarcinoma (EPC) is a rare, aggressive skin cancer arising from eccrine sweat glands, comprising less than 0.01% of all skin cancers. Management is especially complex in immunosuppressed patients due to increased tumor aggressiveness, recurrence, and limited treatment options. We present a 69-year-old woman with recurrent facial EPC following liver and kidney transplantation for Wilson’s disease and hepatitis C. Despite multiple surgeries and two courses of radiation, she experienced multifocal locoregional recurrence. Immunotherapy was contraindicated due to high graft rejection risk, and prior radiation limited options. Radical facial resection with orbital exenteration, bilateral neck dissection, and complex reconstruction using VRAM and pectoralis major flaps, scalp rotation, and skin grafting was undertaken. This case highlights the challenges of treating EPC in immunosuppressed patients and underscores the need for a multidisciplinary approach. While surgery remains the cornerstone of treatment, novel therapies including immune checkpoint inhibitors warrant further study in transplant recipients.
Introduction
Eccrine porocarcinoma (EPC) is a rare, aggressive malignancy originating from the intraepidermal ductal portion of eccrine sweat glands [1–3]. It accounts for approximately 0.005%–0.01% of all cutaneous malignancies [1]. EPC most often presents in elderly individuals, with a median age between 60 and 80 years, and no clear sex predilection [1–3]. It may arise de novo or from a pre-existing benign eccrine poroma [1–3].
The head and neck regions are common sites, followed by the lower extremities and trunk [1–3]. Clinical presentation varies from a painless nodule to an ulcerated, invasive lesion. Due to rarity and overlapping histological features, EPC is often misdiagnosed, delaying treatment [2]. Its aggressive behavior, including perineural invasion, lymphovascular spread, and metastatic risk, makes early diagnosis critical [1–5].
We present a case of recurrent, aggressive facial porocarcinoma in a long-term immunosuppressed patient following renal and hepatic transplants. Organ transplant recipients on chronic immunosuppressants are at increased risk of aggressive skin cancers due to impaired immune surveillance [6]. This case highlights management challenges and the need for a multidisciplinary approach for optimal oncologic and reconstructive outcomes.
Case report
Mrs. AB is a 69-year-old with a recurrent porocarcinoma to the right face. She has an underlying history of immunosuppression for liver and renal transplants for Wilsons Disease and Hepatitis C which she contracted due to a contaminated blood transfusion. She has excellent graft function with normal creatinine, GFR, and liver function tests. Her immunosuppressive regimen includes Tacrolimus and Prednisone. Aside from her transplant-related immunosuppression, she remains in good general health. Her first excision of her right temporal porocarcinoma was in 2021, which showed positive margins and perineural invasion. Follow up computed tomography (CT) also showed an enhancing nodule in the parotid gland. She subsequently had a re-excision of right forehead with full thickness skin graft, right neck lymph node dissection (levels 1, 2, 3), and total parotidectomy. The pathology showed porocarcinoma with positive vascular and perineural invasion with deep margins positive. There was extensive node positive disease in the parotid, and level 2 and 3 nodes. Subsequently treatment with adjuvant radiation included 66 Gy in 33 fractions to the hemiface and neck. In 2023 she developed recurrence medial and inferior to the radiation field and underwent repeat wide local excision, decortication of right frontal skull, and full thickness graft. Pathology returned with positive peripheral and deep margins. A new satellite lesion developed near the medial canthus of the eye that was excised and followed by a second course of radiation.
In 2025, four years from initial surgery, she presented with multifocal recurrence, including an ulcerated periorbital mass, facial edema, and nodal spread (Fig. 1). CT scan demonstrated the frontal and periorbital lesions with enlarged parotid-adjacent nodes (Fig. 2), but no distant metastases. Multidisciplinary consultation concluded that no further radiotherapy was available given her previous treatment. Cytotoxic chemotherapy unlikely to offer benefit. Immunotherapy was contraindicated due to graft rejection risk of nearly 40% and organ failure of 70% [7].

Locoregional recurrence characterized by an ulcerated frontal and periorbital mass, facial edema, and nodal metastases.
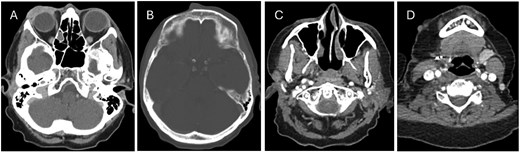
CT head showing (A) right periorbital mass, (B) anterior soft tissue lesion along the forehead medial to the site of prior frontal bone decortication, (C + D) nodal and dermal metastatic deposits within the right neck.
With Surgical Oncology, ENT, and Plastic Surgery coordination, she underwent radical resection including orbital exenteration, radical resection of dermal metastases, bilateral neck dissection, and facial reconstruction with a VRAM free flap, pectoralis major flap, scalp rotation flap, and skin grafting (Fig. 3).

Intraoperative photos demonstrating radical resection including orbital exenteration, resection of dermal metastases, and bilateral neck dissection, followed by facial reconstruction utilizing a free VRAM flap, pectoralis major flap, scalp rotation flap, and skin grafting.
Discussion
EPC presents unique diagnostic and therapeutic challenges due to its rarity, potential for aggressive behavior, and high recurrence rate. Diagnosis relies on histopathological examination and immunohistochemical staining, with EPC typically demonstrating positive staining for epithelial markers such as carcinoembryonic antigen, cytokeratin 7, and epithelial membrane antigen, which help differentiate it from other adnexal and cutaneous malignancies [8, 9]. Dermoscopic evaluation may reveal polymorphic vascular patterns and milky-red areas, aiding in early suspicion [2, 8, 9].
As evident in our case, immunosuppression plays a crucial role in the pathogenesis of aggressive cutaneous malignancies, including EPC. Transplant recipients, particularly those on calcineurin inhibitors or mammalian targets of rapamycin inhibitors, have a higher risk of developing aggressive and recurrent skin cancers [6]. This case underscores the need for close dermatologic and oncologic surveillance in immunosuppressed patients, as well as potential adjustments in immunosuppressive regimens to mitigate oncologic risk.
The standard treatment for EPC is wide local excision with negative margins, as positive surgical margins are a strong predictor of local recurrence [3]. However, given the tumor’s infiltrative nature, Mohs micrographic surgery has been increasingly utilized to achieve precise margin control while preserving healthy tissue [10]. In high-risk cases, such as those with deep invasion, perineural involvement, or regional metastases, adjuvant therapies, including radiation therapy, may be warranted. While there is limited data on the efficacy of chemotherapy and targeted therapies, platinum-based regimens and tyrosine kinase inhibitors have been explored in metastatic cases with variable success [5, 11].
Recent studies have explored the molecular characteristics of EPC, identifying potential therapeutic targets. Next-generation sequencing has revealed mutations in genes such as TP53, HRAS, and PIK3CA, suggesting a potential role for targeted therapies [9, 11]. Immune checkpoint inhibitors, such as PD-1 and CTLA-4 inhibitors, have shown promise in other aggressive cutaneous malignancies, and ongoing clinical trials are evaluating their efficacy in EPC. Immunotherapy, particularly with PD-1 inhibitors, has shown promise in the treatment of advanced EPC [9, 11]. Specifically, pembrolizumab, a PD-1 inhibitor, has been reported to be a promising treatment option for metastatic EPC. A systematic review highlighted the potential of pembrolizumab in treating advanced EPC, although the data is limited. Additionally, molecular profiling of metastatic EPC has indicated that high tumor mutational burden and activation of pathways such as EGFR/MAPK may make these tumors responsive to immune checkpoint inhibitors, including PD-1 inhibitors [9, 11]. However, there is currently no specific mention of CTLA-4 inhibitors being used in the treatment of porocarcinoma. The combination of PD-1 and CTLA-4 inhibitors has shown efficacy in other cancer types, but its application in porocarcinoma remains to be explored further [2, 9, 11].
Extensive facial resection requires complex reconstruction. In this case, the VRAM flap, pectoralis major flap, and scalp rotation flap achieved robust coverage and preserved facial contour and function. Multidisciplinary management was essential for both oncologic and reconstructive success [9, 11, 12].
Conclusion
This case highlights the complexities of managing recurrent, aggressive EPC in an immunosuppressed patient. Integration of multimodal therapies, vigilant surveillance, and advanced reconstruction is key. As research advances, targeted molecular therapies and immunotherapy may transform management of this rare malignancy.
Conflicts of interest
None declared.
Funding
None declared.

{kind=link}
{kind=link}
{kind=link}