





Abstract
This report delineates a case of a 53-year-old male with a fibrin-associated large B-cell lymphoma (FA-LBCL) who initially presented with a large right upper quadrant mass, radiologically suggestive of an 18.6 cm retroperitoneal cystic lesion and biochemically mimicking an atypical pheochromocytoma. The patient underwent laparotomy and removal of the cystic tumour containing 2.5 L of fluid. Final surgical pathology confirmed FA-LBCL, demonstrating the first case of a retroperitoneal cystic FA-LBCL with biochemical changes mimicking an atypical pheochromocytoma.
Introduction
Fibrin-associated large B-cell lymphoma (FA-LBCL) is a rare subtype of lymphoma, considered a distinct neoplasm from diffuse B-cell lymphomas. It is associated with longstanding inflammation and arises within fibrinous material in confined spaces and sites, such as cardiac myxomas, prosthetic devices, breast implants, valvular and vascular grafts, and in pseudocysts of the adrenal, kidney, spleen, and retroperitoneum [1].
Meanwhile, retroperitoneal cystic lesions and adrenal cystic lesions can both harbour various neoplastic and non-neoplastic differential diagnoses, which may mimic one another radiologically [2–4]. Among the differential diagnoses, adrenal cystic pheochromocytoma is a rare possibility as well.
Herein, we present a 53-year-old male whose initial radiologic assessment of his right upper quadrant mass suggested a retroperitoneal cystic tumour, and biochemical workup raised suspicion of a dopamine-secreting lesion. Ultimately, histopathological analysis confirmed a retroperitoneal cyst harbouring FA-LBCL.
Case report
Presentation and investigations
A 53-year-old male is a non-smoker, non-drinker, with type 2 diabetes mellitus and hypertension; he has no prior surgical, endocrinological, or haematological history. On presentation, he was asymptomatic with an incidental finding of anaemia on routine checkup. Clinically, there was a palpable right upper quadrant abdominal mass. Blood pressure was not elevated at presentation, and there were no palpable lymph nodes or other significant findings on physical examination.
Workups were arranged as he was clinically suspected to have a liver mass. Initial blood tests showed a normal liver function test; a normal alpha-fetoprotein (AFP) level, carcinoembryonic-Ag (CEA) level, and CA 19.9 level.
Positron-emission tomography (PET) scan with F18-Fluorodeoxy-glucose (FDG) and C11-Acetate, and combined contrast-enhanced computerized tomography (CT) revealed a predominantly cystic mass measuring ~14.8 × 17.9 × 18.6 cm located on the right side of the abdomen, arising from the retroperitoneal space with close approximation to the adrenal gland. It displaced the adjacent organs, including pancreas and the right kidney; A tiny mural calcification and focal hypermetabolic activity within the cyst wall raised the possibility of malignant transformation (Figs 1–4).
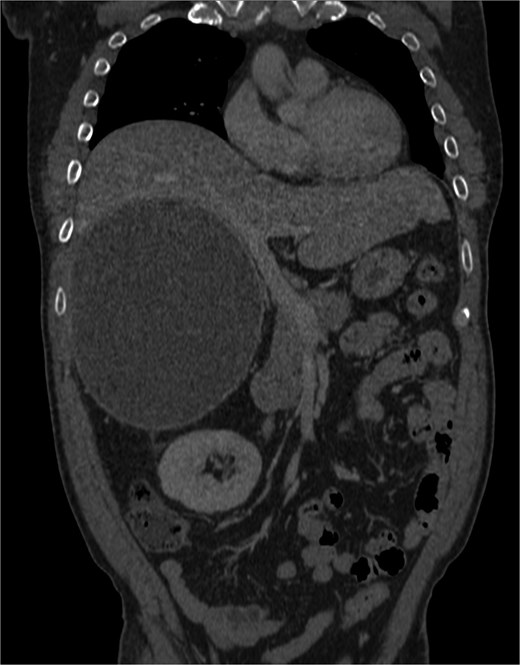
Cystic mass with mural calcification and tissue components in the posteroinferior portion, closely abutting the right kidney and adrenal.

Cystic mass with mural calcification and tissue components in the posteroinferior portion, closely abutting the right kidney and adrenal.

Cystic mass with mural calcification and tissue components in the posteroinferior portion, closely abutting the right kidney and adrenal.
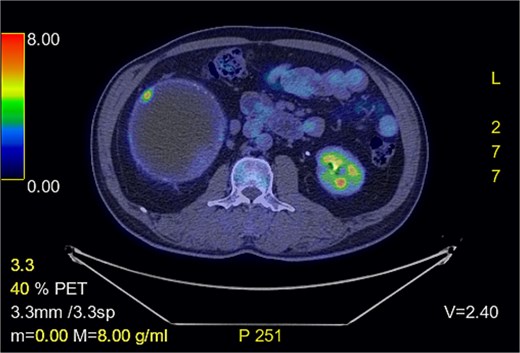
FDG-PET shows focal hypermetabolic activity in the cyst wall.
In view of a possible retroperitoneal tumour, further endocrinological evaluation was done. Chromogranin A level in blood was normal. Two serial 24-hour urine samples collected a few days apart demonstrated elevated dopamine levels (3183 and 2631 nmol/day) (normal: <2468 nmol/day), while noradrenaline, adrenaline, metanephrine, normetanephrine, and 5-hydroxyindoleacetic acid (5-HIAA) levels remained normal.
Based on these findings, the multidisciplinary team decided to manage pre-operatively as a case of atypical pheochromocytoma with appropriate alpha and beta blockade.
Operative findings and procedures
A right subcostal incision was made for laparotomy. A 20 cm right retroperitoneal cystic tumour arising from the right adrenal gland was seen, displacing liver, duodenum, and kidney, with fibrotic adhesion between the tumour, inferior surface of liver, and right kidney.
Due to difficulty in dissection due to limited space, drainage of fluid content from the tumour was performed. A total of 2500 ml purulent fluid was drained, and purse-string suture was applied to the drainage site, and the surrounding area was protected with antiseptic-soaked gauze. The retroperitoneal cystic tumour was resected en bloc with the right adrenal gland.
Pathology
The excised mass included an unilocular cystic lesion containing hemorrhagic material, with no solid area, measuring 17 × 16 × 11 cm, with adrenal gland tissue included.
Microscopic analysis showed a hemorrhagic cyst featuring fibrous cyst wall with haemorrhage and fibrin over the inner surface of the cyst. In scattered areas, there were aggregates of large sized lymphoid cells mixed with fibrin with irregular nuclear membranes and hyperchromatic nuclei. Apoptosis was commonly seen. On immunostaining, they were positive for CD20 and PAX5, with weak heterogeneous staining for CD3, while negative for HHV8. In-situ hybridization for EBER performed returned positive. The lymphoma cells showed no infiltration of adjacent fibroadipose tissue. The background fibrous cyst wall showed lymphoplasmacytic infiltrate with mixed T and B cells with scattered germinal centre formation (CD10+ BCL2-ve). No light chain restriction is noted on kappa and lambda. The background adrenal gland was unremarkable.
In conclusion, the histological features are similar to prior cases of FA-LBCL arising from retroperitoneal pseudocyst [5–7], with scant tumour cells embedded within the fibrous cystic wall, but without the extensive necrotic background.
The aspirated fluid was also sent for cytology and culture, of which cytology showed no evidence of malignancy, and cultures (including for mycobacterium) returned negative.
Patient’s urine dopamine level has also normalized a few months after the operation.
Discussion
FA-LBCL is a highly heterogeneous, distinct disease entity associated with EBV that commonly occurs in chronic fibrinous deposits, previously classified as a subtype of DLBCL associated with chronic inflammation. It presents usually as microscopic lesions, found during pathological analysis, without visible mass formation, with a relatively indolent clinical course compared to DLBCL. It has variable presentation sites, such as in cardiac myxomas, in prosthetic devices, breast implants, cardiac valves, vascular grafts, and in pseudocysts, including adrenal, kidney, spleen, and retroperitoneum [1]. There is no consensus available on whether optimal treatment includes only resection alone or with adjuvant chemotherapy such as R-CHOP, and majority of the cases have been reported in case reports or series only, with <100 cases in English literature [8, 9].
Upon focused review of previously published pathological confirmed case reports of retroperitoneal or adrenal FA-LBCL, majority of cases presented with an incidental finding of a mass either clinically or radiologically without endocrinologic symptoms or workups [1, 5, 8].
As this case’s pathology is not suggestive of a dopamine-secreting tumour (e.g. retroperitoneal paraganglioma, or ganglioneuroma), the cause of elevated urine dopamine is uncertain; In a 2004 case report of a retroperitoneal malignant fibrous histiocytoma mimicking pheochromocytoma, authors attributed the elevated dopamine levels to be due to compression of renal vessels by mass effect seen intra-operatively [10]; A 2019 case report of retroperitoneal seminoma with elevated catecholamines attributed the cause to entrapped ganglion on pathological analysis [11]. Both are not seen in this case, and further studies are needed to demonstrate if and how non-secretory retroperitoneal tumours can lead to changes in catecholamine levels.
To the best of our knowledge, this is the first report of a FA-LBCL in retroperitoneal cystic lesion biochemically mimicking a functional dopamine-secreting adrenal tumour; and endocrinological workup and multidisciplinary management for future cases should also be considered.
Conflicts of interest
None declared.
Funding
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}