





Abstract
Pyogenic granuloma (PG) is a common reactive vascular hyperplasia of the oral cavity with multifactorial origin. Although benign, it shows clinical variability and may recur if predisposing factors persist. This report describes two oral PG cases with different etiologies. A 68-year-old man presented with a mucogingival lesion associated with dental calculus, while a 29-year-old woman developed a lesion during pregnancy that continued after delivery. Both were treated with complete surgical excision and elimination of local irritants. Histopathology confirmed PG, characterized by granulation tissue rich in vascular spaces, inflammatory infiltrate, and areas of epithelial ulceration. Follow-up visits showed good healing and no recurrence. These cases emphasize the interaction of local agents like calculus and biofilm with systemic factors such as gestational hormonal changes. PG management requires identifying contributing factors and performing thorough surgical removal, though alternative methods—cryosurgery, electrosurgery, or laser—may be useful in selected scenarios.
Introduction
Pyogenic granuloma (PG) is a benign vascular condition triggered as a reactive response to certain local or systemic stimuli, including dental biofilm accumulation, trauma, hormonal factors, or chronic irritants [1, 2]. It is considered one of the most common reactive hyperplasias of the oral cavity and, despite its name, is not associated with purulent processes nor does it histologically constitute a true granuloma, which is why the term is considered inappropriate in the specialized literature [1, 3].
From a topographical point of view, oral PG occurs with a particular predilection for the gums, particularly in the anterior sector of the upper jaw, but it can also be found in other areas such as the tongue, lips, oral mucosa, and palate [4]. From a clinical point of view, it is generally identified as an exophytic, pedunculated, or sessile tumor, characterized by a smooth or lobulated surface that is reddish to purplish in color, with a tendency to bleed and, in certain cases, functional discomfort or inconvenience. This condition shows a marked tendency to affect females and can manifest at any stage of life, with a significant preference in the second and third decades [3].
From a therapeutic point of view, surgical excision combined with the removal of local triggering factors is the most commonly used treatment [4, 5]. However, various alternatives have been suggested, such as cryosurgery, laser, electrocautery, or sclerotherapy [3, 6–8]. Despite this, to date there is no standardized protocol for the specific management of oral PG, which highlights the need to describe, analyze, and document new cases.
The aim of this manuscript is to present two clinical cases of oral PG in adult patients, detailing the clinical characteristics and therapeutic management implemented, with the purpose of providing evidence that enriches the understanding and approach to this lesion.
Case report
Clinical case 1
A 68-year-old male patient with no pathological history and healthy periodontium visited the dental clinic with the following complaint: ‘I have a lump on my gum that I bite when chewing.’ Intraoral examination revealed a mucogingival tissue growth on the attached gum, which was firm, oval, fibrous, smooth, and without signs of active ulceration, measuring ~1.1 × 1.0 cm. The lesion originated at the base of the papilla and part of the adjacent masticatory mucosa, presenting a pedunculated base that extended to the interproximal region of teeth 43 and 42, with erythematous coloration and whitish areas (Fig. 1a and b). The patient reported difficulty chewing, with no pain or history of trauma or surgery in the area. A digital periapical radiograph was performed to rule out periodontal or infectious pathology at the bone level.
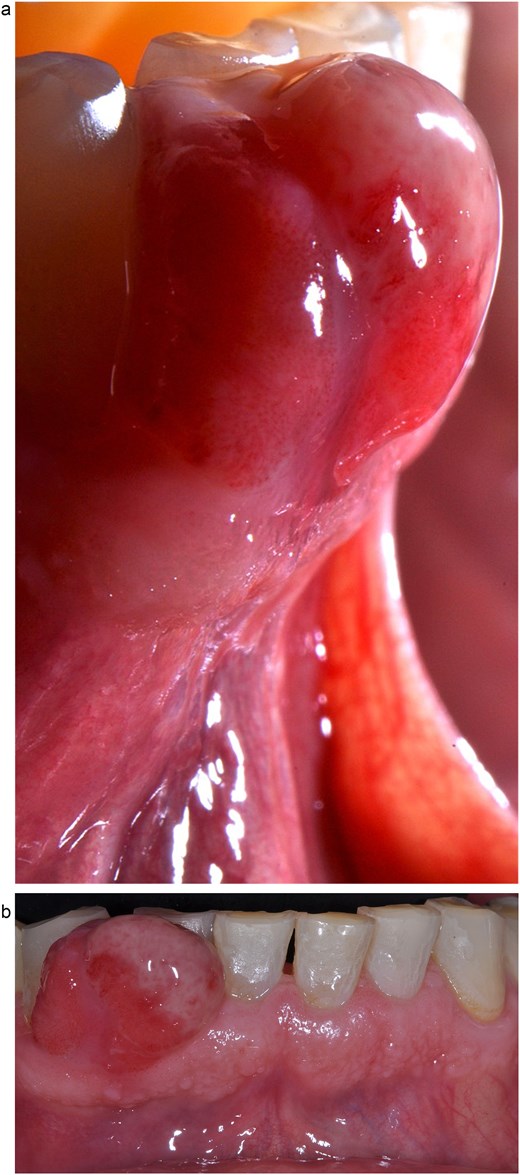
Clinical image of mucogingival tissue growth in the attached gingiva, with a firm, oval, fibrous, smooth appearance and no signs of active ulceration. (a) Lateral view. (b) Frontal view.
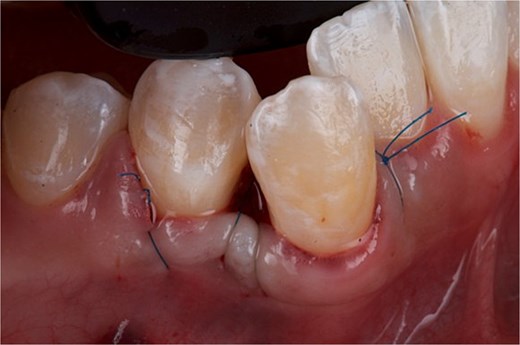
The surgical intervention was aimed at complete removal of the hyperplastic lesion, with the objective of obtaining a definitive diagnosis through histopathological analysis and, simultaneously, eliminating the pathological tissue. Under aseptic and antiseptic conditions, local anesthesia was administered with 4% articaine with epinephrine 1:100 000. Subsequently, using a 15c scalpel blade, the base of the hyperplastic tissue was resected up to the interproximal area of teeth 43 and 42, ensuring adequate margins to guarantee complete removal of the lesion. Dental calculus was identified and removed from the teeth. Next, bone carving was performed with a Kirkland periodontal chisel. The removed tissue was placed in 10% formalin and sent for histopathological study. To promote edge approximation and achieve primary healing, sharp dissection was performed, and the wound was sutured with 5–0 nylon using simple stitches (Fig. 2). Antibiotic therapy (amoxicillin 750 mg every 12 hours for 7 days), analgesic (ibuprofen 600 mg every 8 hours for pain) and rinses with 0.12% chlorhexidine for 15 days were indicated.

Front view of the clinical image of the removal of the intraoral lesion with a 5-zero nylon suture and simple stitches.
The definitive diagnosis was a PG. Histopathological analysis revealed proliferation of granulation tissue consisting of numerous lymphatic and vascular spaces of different sizes, some congestive, accompanied by severe diffuse chronic inflammatory infiltrate composed of plasma cells, lymphocytes, and histiocytes. The stroma showed abundant collagen fibers arranged loosely and irregularly. An ulcer with loss of epithelial continuity and eosinophilic material compatible with fibrin was also observed (Fig. 3a and b). Histological micro-section stained with hematoxylin and eosin (H&E).
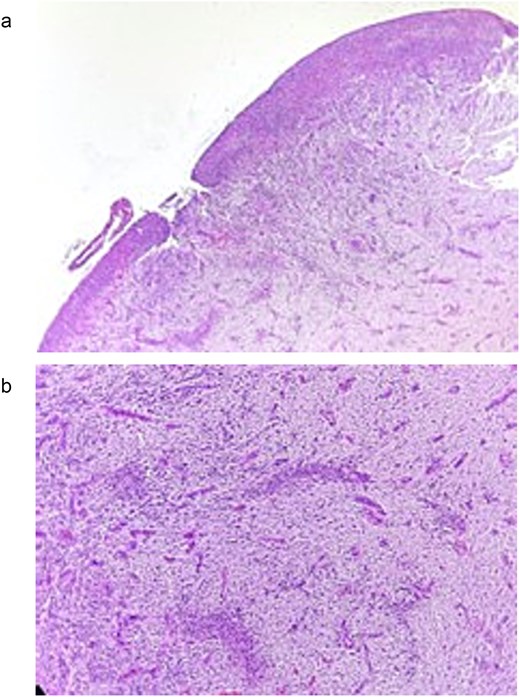
(a) Histological micro-section stained with H&E, showing loss of epithelial continuity and the presence of eosinophilic material consistent with fibrin corresponding to an ulcer. (b) H&E-stained histological micro-section showing granulation tissue consisting of lymphatic and vascular spaces of varying sizes, severe diffuse chronic inflammatory infiltrate, in a stroma of abundant collagen fibers arranged in a loose and irregular manner.
At the 15-day follow-up, adequate secondary healing at the interproximal level and favorable recovery of the soft tissues were evident. The sutures were removed without signs of inflammation, infection, or complications (Fig. 4a and b). In subsequent check-ups, tissue stability was verified, and digital periapical radiographs were taken to rule out recurrence of the lesion. The patient’s adherence to postoperative instructions was crucial to achieving optimal results.
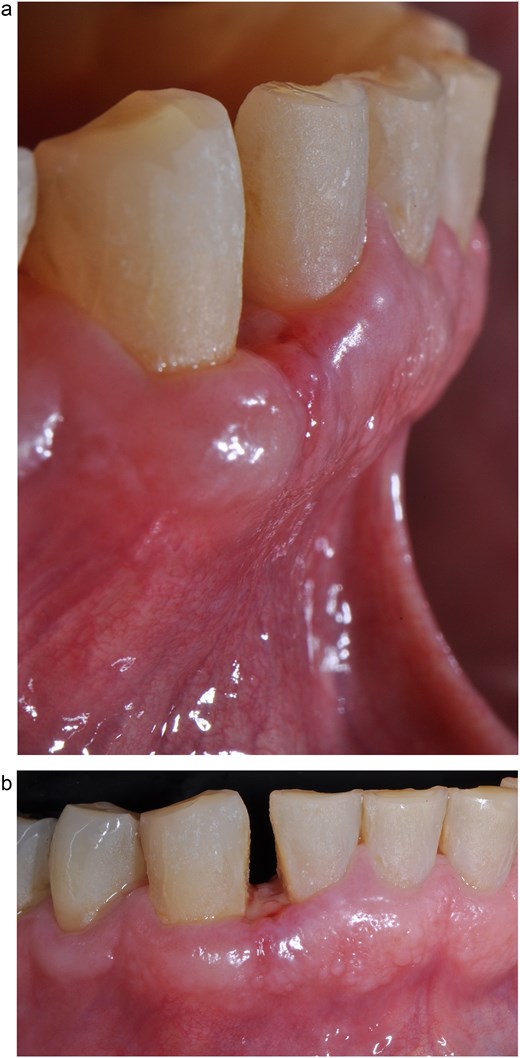
Suture removal 15 days postoperatively. (a) Lateral view. (b) Frontal view.
Clinical case 2
A 29-year-old female patient with no pathological history and healthy periodontium visited the dental clinic with the following complaint: ‘When I was pregnant, a small lump appeared on my gum that bled and would not go away.’ Intraoral examination revealed a mucogingival tissue growth on the attached gum, which was firm, oval, fibrous, smooth, and without signs of active ulceration, measuring ~ 1 × 0.5 cm. The lesion originated at the base of the papilla and part of the adjacent masticatory mucosa, presenting a pedunculated base that extended to the interproximal region of teeth 43 and 44, with erythematous coloration and whitish areas (Fig. 5). The patient reported pain on palpation, with no history of trauma or surgery in the area. A digital periapical radiograph was taken to rule out periodontal or infectious pathology at the bone level.

Front view of the clinical image of the intraoral lesion: Growth of mucogingival tissue in the attached gingiva, with a firm, oval, fibrous, smooth appearance and without signs of active ulceration.
The surgical intervention was aimed at completely removing the hyperplastic lesion, with the objective of obtaining a definitive diagnosis through histopathological analysis and, simultaneously, eliminating the pathological tissue. Under aseptic and antiseptic conditions, local anesthesia was administered with 4% articaine with epinephrine 1:100 000. Subsequently, using a 15c scalpel blade, the base of the hyperplastic tissue was resected up to the interproximal area of teeth 43 and 44, ensuring adequate margins to guarantee complete removal of the lesion. Bone carving was then performed with a Kirkland periodontal chisel. The removed tissue was placed in 10% formalin and sent for histopathological study. To promote edge approximation and achieve primary healing, sharp dissection was performed, the flap was elevated to the mesial part of OD 43, and the wound was sutured with 5–0 nylon using simple stitches and a suspension stitch (Fig. 6). Antibiotic therapy (amoxicillin 750 mg every 12 hours for 7 days), analgesic (ibuprofen 600 mg every 8 hours for pain) and rinses with 0.12% chlorhexidine for 15 days were indicated.
Front view of the clinical image of the removal of the intraoral lesion with simple 5-point nylon suture and suspension stitches.
The definitive diagnosis was a PG. Histopathological analysis revealed hyperplasia of the granulation tissue consisting of abundant blood capillaries, some congested, accompanied by moderate diffuse mixed inflammatory infiltrate, composed of plasma cells, lymphocytes, and histiocytes, as well as numerous young fibroblasts on a stroma of collagen fibers arranged loosely and irregularly. The lesion was covered by non-keratinized stratified squamous epithelium, which showed leukocyte exocytosis, spongiosis, and pseudoepitheliomatous hyperplasia. Additionally, in one field, loss of epithelial continuity, eosinophilic material with fibrin, mixed inflammatory infiltrate, and cellular debris compatible with ulceration were observed (Fig. 7a–c).
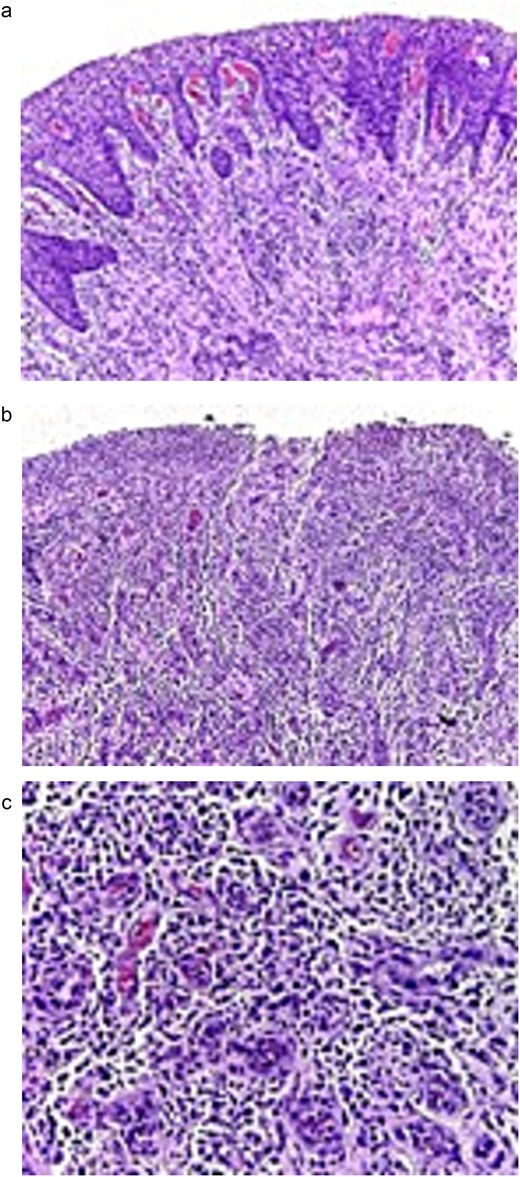
Histological micro-sections stained with H&E. (a) The lesion is covered by a stratified squamous epithelium that is not keratinized, which exhibits signs associated with inflammation (10×). (b) Towards one field, there is a loss of epithelial continuity consistent with ulceration (10×). (c) At higher magnification, hyperplasia of granulation tissue is observed, consisting of numerous blood capillaries, some with erythrocytes in their lumen, severe mixed inflammatory infiltrate, fibroblasts, and collagen fibers.
At the 15-day follow-up, adequate secondary healing at the interproximal level and favorable soft tissue recovery were evident. The sutures were removed without signs of inflammation, infection, or complications (Fig. 8). In subsequent check-ups, tissue stability was verified, and digital periapical radiographs were taken to rule out recurrence of the lesion. The patient’s adherence to postoperative instructions was crucial in achieving optimal results.

Front view of the clinical image of suture removal 15 days postoperatively.
Discussion
Diverse local and systemic stimuli have been identified as triggers in the genesis of PG, which explains its high incidence in the oral cavity, accounting for between 24% and 50% of the reactive hyperplasias described [2]. The etiology is multifactorial and constitutes the basis of its pathogenesis: chronic irritation caused by repetitive mechanical aggression, dental biofilm, and hormonal variations at different stages such as puberty and pregnancy are recognized as key triggers [1, 2, 9, 10]. In turn, certain drugs, including immunosuppressants (cyclosporine, tacrolimus) and calcium channel blockers (nifedipine), have been linked to its genesis by stimulating abnormal fibrovascular proliferation.
In the first case, the clinical finding was linked to the accumulation of dental calculus, which represents a persistent irritant that triggers the hyperplastic process. The literature has extensively described how this type of stimulus is one of the primary triggers of PG, because dental biofilm and calculus deposits induce a sustained inflammatory response that stimulates fibrovascular proliferation, contributing to its reddish appearance and tendency to bleed [5]. In this same context, Sharma et al. (2019) and Lomelí et al. (2023), highlight that chronic irritation caused by dental biofilm or defective restorations stimulates a disproportionate tissue reaction, leading to the formation of highly angiogenic granulation tissue [1, 2]. Our patient’s clinical case showed this etiological pattern, as he had no history of systemic conditions or predisposing factors other than calculus, highlighting the importance of adequate periodontal control and the removal of local irritants as a preventive measure for these conditions. In contrast, the second case of the female patient presented a completely different scenario, as the condition originated during pregnancy. Hormonal variations play a fundamental role in the pathogenesis of PG [9, 11]. During pregnancy, the significant increase in estrogen and progesterone enhances vascular proliferation and alters immunoregulation, stimulating an inflammatory microenvironment [11, 12]. These changes explain why oral PGs during pregnancy are characterized by accelerated growth, a reddish appearance, and a marked tendency to bleed, as in our case. Several studies have shown that, although some pregnancy-induced granulomas tend to disappear spontaneously after delivery, a considerable number persist and require therapeutic intervention for resolution [2, 12]. Accordingly, our case is similar to that described by Meshram et al. (2023), highlighting that post-gestational persistence requires active intervention to prevent complications [5].
With regard to therapeutic alternatives, conventional surgical removal continues to be the most widely used first-line treatment, allowing a sample to be obtained for histopathological analysis and ensuring adequate margins; this technique was used in the two cases presented [2, 13]. However, this modality has disadvantages, such as intraoperative bleeding and slower healing [13]. In order to overcome these limitations, various techniques with different characteristics have been implemented over the years [3, 6–8]. Diode, CO₂, and Er: YAG lasers are techniques that offer superior hemostatic control, less oedema, and a faster healing period, making them particularly useful in patients with systemic conditions such as diabetes mellitus. On the other hand, cryosurgery and electrosurgery are less invasive procedures for small or moderate entities, with shorter surgical times and satisfactory pain control [2]. Sclerotherapy with agents such as sodium tetradecyl sulphate or polidocanol, described by Soni et al. (2021), is a conservative, effective, and economical therapeutic option, particularly indicated for extensive lesions or those located in aesthetic areas, as it reduces the risk of bleeding and recurrence [6]. The choice of therapeutic strategy should be tailored to each individual case according to the location, size of the lesion, the patient’s systemic conditions, and aesthetic considerations, bearing in mind that all therapeutic modalities aim not only to remove the lesion but also to reduce the possibility of recurrence by controlling predisposing etiological factors.
At the same time, it is important to emphasize preventive measures such as the complete removal of local irritants and proper oral hygiene, as recurrence remains one of the most significant complications of oral PG [1, 2]. Several studies have shown that the recurrence rate can be as high as 16% of cases, particularly when adequate margins are not considered in surgical removal or when certain triggering factors such as dental calculus, chronic trauma, or inadequate restorations persist. Other causes have also been considered, including angiopoietin 1 and 2, ephrin B2, hormone levels, viral oncogenes, microscopic arteriovenous malformation, and fibroblast gene depression [2, 12, 14]. From this perspective, the elimination of local irritants and the implementation of an adequate oral hygiene program have become fundamental determinants for reducing the recurrence of the condition. Additionally, it has been shown that cases linked to changes in hormonal levels have a greater tendency to recur in the absence of control of gingival inflammation or persistence of dental biofilm. Consequently, therapeutic success does not depend exclusively on the technique implemented (sclerotherapy, laser, or surgical intervention), but also on proper clinical follow-up and the patient’s active participation in controlling local factors. Thus, the prevention of recurrence is a fundamental pillar in the management of oral PG, alongside the choice of therapeutic management.
Consequently, the two clinical cases presented show that different etiological factors, whether the presence of local irritants such as dental calculus or hormonal imbalances caused by pregnancy, converge in the same clinical and histopathological manifestation, originating from different pathogenic processes. This parallelism highlights the need for therapeutic management to consider both the identification of local triggers and systemic and hormonal conditions. Additionally, it reaffirms that understanding the etiology of this lesion is essential for designing an appropriate therapeutic plan and for applying preventive strategies against recurrence.
These clinical cases demonstrate the multifactorial nature of oral PG, showing that persistent irritants and systemic changes can trigger this vascular condition. The contrast between the two scenarios highlights the importance of the clinical and diagnostic approach considering the detection of mechanical irritants and the exploration of hormonal or systemic conditions that contribute to the genesis of the lesion.
With regard to the therapeutic approach, conventional surgical intervention together with the removal of predisposing factors remains the treatment of choice. However, various alternatives such as cryosurgery, laser, electrosurgery, or sclerotherapy have benefits in some cases, particularly in patients with comorbidities or aesthetic concerns. It is essential to emphasize that the success of treatment for this condition is not exclusive to the technique implemented, but rather to the control of etiological agents and adequate clinical follow-up.
Author contributions
Francisco Javier Alcaraz-Baturoni (Writing—review & editing), Jessica Paola Ibarra-González (Writing—review & editing), Mario Alberto Alarcón-Sánchez (Conceptualization, Validation, Methodology, Writing—original draft, Writing—review & editing), Giselle Berenice Vela-Sancho (Conceptualization, Validation, Methodology, Writing—original draft, Writing—review & editing), Javier Flores-Fraile (Ssupervision, Conceptualization, Writing—original draft, Writing—review & editing), Artak Heboyan (Supervision, Conceptualization, Writing—Original draft, Writing—review & editing), Rocio Del Carmen Anaya-Macías (Writing—review & editing), and Sarah Monserrat Martínez-Lomelí (Formal analysis, Investigation, Conceptualization, Project administration, Writing—original draft, Writing—review & editing)
Conflicts of interest
All authors have no conflicts of interest to disclose.
Funding
None declared.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Patient informed consent
The patient reported in this manuscript provided written informed consent for the publication of the case details.
CARE Checklist (2016) statement
The authors have read the CARE Checklist (2016), and the manuscript was prepared and revised according to the CARE Checklist (2016).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}