





Abstract
Acute intrathoracic sigmoid volvulus secondary to major congenital atic eventration in an adult is exceptionally rare. We report the case of an 18-year-old male with lifelong constipation who presented an acute bowel obstruction caused by intra thoracic sigmoid volvulus in major left diaphragmatic eventration. Despite complete functional loss of the left lung, the patient had no significant respiratory complaints. Emergency endoscopic decompression was performed, followed by sigmoidectomy and diaphragm plication, preventing recurrence of volvulus and improving respiratory function. This case highlights that longstanding constipation and subtle respiratory limitation since childhood were warning signs that could have prompted earlier diagnosis and management of diaphragmatic eventration, potentially preventing the acute presentation.
Introduction
Acute bowel obstruction revealing a major congenital diaphragmatic eventration is exceptionally rare in adults. Prior to such an acute presentation, symptoms may be underestimated during childhood, often limited to chronic constipation or atypical abdominal pain [1]. These symptoms may correspond to episodes of spontaneously reversible partial sigmoid volvulus [2, 3]. When not identified at birth, diaphragmatic eventration can progressively enlarge due to constitutional muscular hypoplasia, creating a wide thoracoabdominal compartment. We report the exceptional case of a young, non-sportive adult presenting with acute colonic obstruction without significant respiratory symptoms, despite a complete functional loss of his left lung.
Case presentation
An 18-year-old male originally from Egypt presented to the emergency department with severe abdominal pain suggestive of bowel obstruction. Over the preceding 10 days, he had experienced recurrent non-bilious vomiting, and bowel movements had ceased for 48 h. Since childhood, he had suffered from frequent constipation and had developed chronic abdominal pain during the past year. He had never engaged in sports, particularly endurance activities, and had taken no chronic medication other than laxatives. Physical examination revealed a markedly distended abdomen and absence of breath sounds on the left side. Contrast-enhanced chest and abdominal computed tomography (CT) demonstrated a mesentero-axial sigmoid volvulus with a characteristic “whirl sign,” without evidence of perforation (Fig. 1A and B). The most distended segment of colon had migrated into a large left diaphragmatic eventration, causing mediastinal shift and complete left lung atelectasis (Figs 1C and 2A). Laboratory tests showed no inflammatory response. Under general anesthesia, an initial bedside endoscopic decompression achieved partial detorsion, requiring a second successful endoscopic procedure. Owing to the presence of megacolon and marked mesenteric laxity, the risk ofrecurrence remained high, and surgical management was indicated. Due to organizational constraints, a two-step surgical strategy was adopted. First, an open sigmoidectomy with mechanical end-to-endcolorectal anastomosis was performed. Before thoracic correction, dynamic thoracic magnetic resonance imaging confirmed persistent massive eventration (Fig. 3A), with major mediastinal displacement and absence of contractile activity of the left hemidiaphragm. Pulmonary function tests showed an forced expiratory volume in one second at 71% of predicted (decreasing to 64% in the supine position) and a vital capacity of 74%. Two months later, diaphragm plication reinforced with prosthetic mesh was performed through a video-assisted lower lateral mini-thoracotomy. Intraoperative findings confirmed a massive eventration leaving minimal space for the compressed left lung (Fig. 3B). The diaphragm was extremely thin—~1 to 2 mm—appearing nearly transparent after incision (Fig. 3C). Postoperative recovery was uneventful, except for a transient functional bowel obstruction managed medically. Histopathologic examination of the resected colon ruled out Hirschsprung disease and revealed chronic ischemic changes with fibrosis separating the external muscular layer (Fig. 3D). Four months after the final procedure, the patient showed clear clinical improvement, with normalized bowel habits and the ability to climb several flights of stairs without dyspnea. Chest X-ray confirmed left lung re-expansion and mediastinal repositioning (Fig. 2B). Chronic colonic distension persisted without symptoms and exerted mild upward pressure on the repaired left hemidiaphragm.
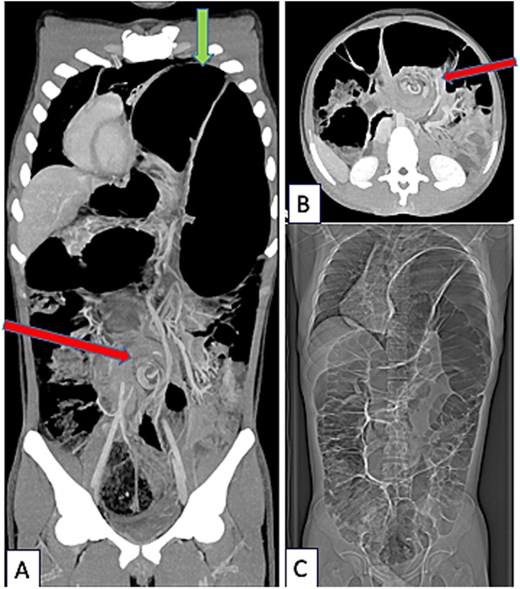
CT-scanner thoracic abdominal and pelvic at portal phase (Siemens X-Cite 2021 Healthcare Erlangen Iomeron 350), coronal (A) and axial view (B). Sigmoid Volvulus with pathognomonic Whirl Sign (arrow in the middle of figures A and B) associated with severe diaphragmatic eventration (arrow at the top of figure A). Complete coronal view (C): global colonic distention.
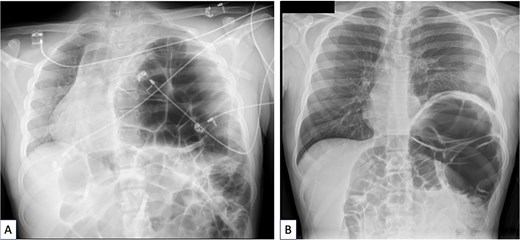
(A) Chest X-ray done when acute sigmoid volvulus occurred, revealing the major diaphragmatic eventration causing severe contralateral mediastinal shift and complete left lung atelectasis. (B) Chest X-ray done 4 months after sigmoidectomy and diaphragm plication. The left lung is well reexpanded and the mediastinum is in good position. The left hemidiaphragm is stabilized at a correct but high level because of persistent megacolon despite sigmoidectomy.
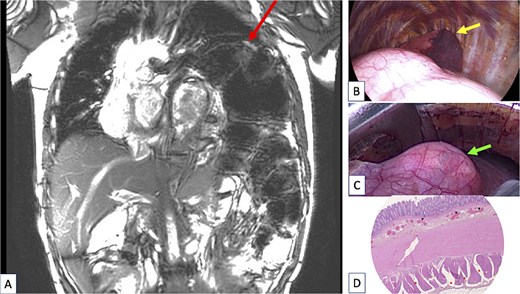
(A) Coronal view of the chest magnetic resonance imaging done after sigmoidectomy showing a huge persistent left diaphragmatic eventration (arrow at the top of figure) containing the remaining large megacolon. The left lung was totally compressed in the upper part of the pleural cavity and a severe mediastinal shift persisted despite digestive surgery. (B) Peroperative view of the thoracic procedure showing the major diaphragm eventration pushing the lung (arrow showing lung) in the upper part the pleural cavity. The lung is almost in full atelectasis. (C) Peroperative view of the thoracic procedure showing a “transparent diaphragm” (arrow showing thin diaphragm) without muscle consistence. (D) Histopathologic examination of the resected colon, using haematoxylin and eosin (H&E) staining. Cross section of the colonic wall (H&E—2.5×) showing small congestive vessels within the submucosal layer (black triangles) and fibrosis dissociating the external muscular layer (red triangles).
This study received no specific funding. Written informed consent was obtained from the patient for publication.
Discussion
The association of sigmoid volvulus with major congenital diaphragmatic eventration is extremely rare in adulthood. In this case, acute colonic obstruction uncovered two congenital abnormalities: left hemidiaphragm eventration and megacolon with mesenteric laxity. Neither condition had been recognized during childhood, although longstanding warning signs should have prompted earlier evaluation. Congenital diaphragmatic eventration is a rare malformation in which part of the diaphragm is replaced by fibroelastic tissue [1]. The combination of diaphragmatic eventration and gastric volvulus is more frequently described and represents a true surgical emergency [4–6]. The diagnosis relies on Borchardt’s triad—severe epigastric pain, unproductive retching, and inability to pass a nasogastric tube. Only a few cases of sigmoid volvulus occurring within a diaphragmatic eventration have been reported, and all followed prolonged periods of chronic constipation likely corresponding to subacute volvulus episodes [1, 2]. Two main factors predispose to volvulus in this setting: A large supra-abdominal space created by eventration, facilitating colonic migration and twisting, and a long, lax mesenteric pedicle.
Whether eventration can be a consequence of chronic constipation, as suggested by Yoshimori et al. [3], or whether both anomalies coexist congenitally remains debated. Outside of diaphragmatic anomalies, endoscopic decompression is recommended as first-line treatment in sigmoid volvulus, with success rates near 80% [6, 7]. However, volvulus associated with diaphragmatic eventration is considered a surgical emergency requiring operative correction [8]. Approximately 18% of patients with sigmoid volvulus have underlying Hirschsprung disease, which justifies systematic histopathologic analysis of the resected colon [9].
Diaphragm plication is the recommended treatment for symptomatic eventration. In congenital cases, muscular atrophy is often severe, supporting prosthetic reinforcement. In the only available comparative series, recurrence was more frequent when plication was performed without mesh reinforcement [10]. Early identification and treatment of diaphragmatic eventration in children with atypical respiratory and digestive symptoms could prevent severe complications such as digestive volvul0us.
Conclusion
Acute sigmoid volvulus revealing major congenital diaphragmatic eventration is exceptionally rare in adulthood. Management requires treating both abnormalities, either in a single or staged procedure. The surgical strategy should aim to restore a durable thoracoabdominal barrier. Early recognition in childhood, particularly in patients with chronic constipation and exercise-induced respiratory limitation, may prevent life-threatening complications.
Conflicts of interest
None declared.
Funding
None declared.

{kind=link}
{kind=link}
{kind=link}