





Abstract
A 71-year-old diabetic man presented with progressive cholestatic jaundice secondary to a Bismuth II hilar cholangiocarcinoma. Surgical exploration revealed a tumor confined to the biliary confluence. A limited en bloc resection of the confluence with multiple biliary reconstructions by end-to-side hepaticoduodenostomy was performed without hepatic resection. The postoperative course was uneventful. This case illustrates the feasibility of limited hilar resection with direct biliary reconstruction in selected frail patients when extended hepatectomy is contraindicated.
Introduction
Hilar cholangiocarcinoma (HCCA) represents ~60% of bile duct malignancies and remains one of the most technically demanding pathologies in hepatobiliary surgery [1]. While standard curative management relies on major hepatectomy with biliary reconstruction, morbidity, and postoperative mortality remain significantly elevated in elderly or comorbid patients, frequently limiting the feasibility of radical resection [2].
In selected vulnerable patients with preserved segmental ductal anatomy, limited resection of the biliary confluence combined with direct biliary-enteric reconstruction may offer a meaningful oncologic compromise, reducing surgical trauma while maintaining ductal patency [3].
We present a case illustrating this approach in a frail diabetic patient with Bismuth II HCCA.
Case report
A 71-year-old man with insulin-dependent diabetes presented with a 40-day history of progressive jaundice, pruritus, and weight loss. Laboratory tests showed cholestasis without hepatic failure.
Preoperative work-up:
The Eastern Cooperative Oncology Group (ECOG) performance status: 2
Charlson comorbidity index: 7 (age + insulin-treated diabetes + cardiovascular risk)
The albumin-bilirubin (ALBI) grade 2 with estimated future liver remnant <30%.
These parameters classified the patient as non-optimal for major hepatectomy, and a less extensive surgical strategy was considered.
Computed tomography and magnetic resonance cholangiopancreatography (Supplementary Videos 1 and 2) demonstrated intrahepatic bile duct dilatation with a focal thickening at the biliary confluence, consistent with Bismuth II Klatskin tumor. No vascular invasion or distant metastasis was identified.
Operative findings
Through a right subcostal incision, complete Kocher maneuver exposed the hepatic hilum. The hepatoduodenal ligament was dissected, and the common hepatic duct was isolated up to the bifurcation.
The hilar plate was approached anteriorly, revealing tumor involvement limited to the confluence.
A monobloc resection of the biliary confluence was performed (Figs 1 and 2). The right system was divided distal to its bifurcation (segments I, V–VIII, VI–VII branches individually). The left duct was divided at its origin.
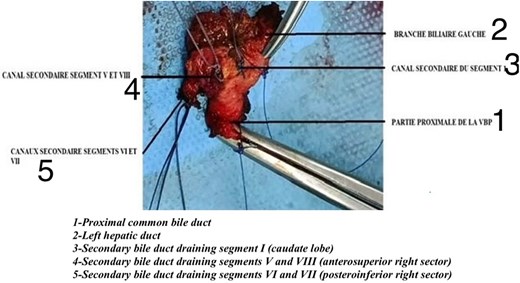
Resected specimen, 1. Proximal common bile duct/2. Left hepatic duct/3. Secondary bile duct draining segment I (caudate lobe)/4. Secondary bile duct draining segments V and VIII (anterosuperior right sector)/5. Secondary bile duct draining segments VI and VII (posteroinferior right sector).
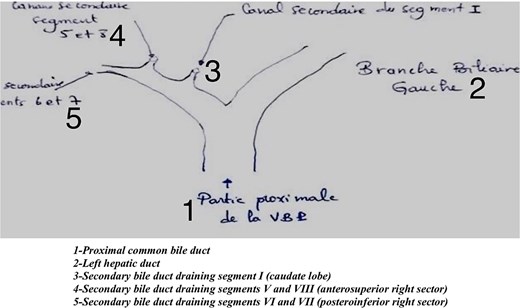
Illustrative figure of the resected specimen, 1. Proximal common bile duct/2. Left hepatic duct/3. Secondary bile duct draining segment I (caudate lobe)/4. Secondary bile duct draining segments V and VIII (anterosuperior right sector)/5. Secondary bile duct draining segments VI and VII (posteroinferior right sector).
Reconstruction consisted of an end-to-side hepaticoduodenostomy encompassing the left duct and right sectoral ducts using interrupted 4-0 PDS sutures.
A biopsy of adjacent liver confirmed tumor-free parenchyma. No drain was left. The postoperative course was uneventful, and the patient was discharged on Day 8.
Technical note
The duodenum was mobilized up to the genu superius to achieve tension-free anastomosis.
A single-layer interrupted mucosa-to-mucosa suture was used.
Intraoperative bile duct calibration allowed functional alignment of the ducts to the duodenum without rotation.
Discussion
Complete (R0) resection remains the cornerstone of curative intent for HCCA [1, 4]. However, extensive hepatectomy carries up to 20%–30% postoperative morbidity and mortality in fragile patients [5]. This risk is particularly relevant in elderly, comorbid, or diabetic patients, where liver regeneration capacity and cardiorespiratory reserve are frequently reduced, making extended hepatectomy unsuitable.
Recent series suggest that limited hilar resection can achieve R0 margins in selected Bismuth I–II lesions [2, 6]. In such cases, limited resection may represent a more physiologically acceptable alternative, especially when preoperative frailty scoring or volumetric assessment predicts high morbidity after major hepatectomy.
In our patient, the indication for confluence-limited resection was guided by a high frailty profile (age, insulin-dependent diabetes) and by anatomic resectability criteria confirming absence of vascular involvement. This reflects a growing trend toward individualized tailoring of surgical aggressiveness to biological reserve rather than tumor anatomy alone.
Reconstruction strategy
Roux-en-Y hepaticojejunostomy has long been the gold standard, but direct hepaticoduodenostomy (HD) offers shorter operative time, physiological bile flow, and easier postoperative endoscopic access [3, 7]. These advantages are particularly valuable in frail or elderly patients who may not tolerate longer operative durations or future reintervention via jejunal access.
Comparative studies demonstrate no significant difference in long-term anastomotic patency between HD and hepaticojejunostomy [8].
A recent review confirmed the safety of HD after complex bile duct resections in non-infected fields [9].
According to the 2025 NCCN guidelines, the reconstructive choice should be individualized based on tumor extent, patient condition, and surgeon experience [10]. Our case aligns with this recommendation, demonstrating that limited resection with HD can achieve biliary continuity with low morbidity when major hepatectomy carries prohibitive surgical risk.
Learning points
Limited confluence resection may achieve R0 in selected Bismuth II hilar cholangiocarcinoma.
Hepaticoduodenostomy is a safe, physiological alternative to Roux-en-Y reconstruction.
Intraoperative duct mapping and precise suture orientation are crucial for long-term patency.
Individualized surgical strategies are essential in frail or comorbid patients.
Conclusion
Limited biliary confluence resection followed by hepaticoduodenostomy represents a viable, organ-preserving oncologic option in frail, comorbid, or elderly patients with Bismuth II HCCA when major hepatectomy is contraindicated.
This case demonstrates that oncologic clearance can be achieved while reducing surgical stress, provided selection criteria are strict, anatomy favorable and reconstruction performed with high technical precision.
Long-term outcome data and prospective validation remain required before broad adoption, but in carefully chosen profiles, this strategy may meaningfully expand access to curative-intent surgery.
Conflict of interest statement
None declared.
Funding
None declared.
References
Benson 3rd AB, D’Angelica MI, Abrams T, et al. . Biliary tract cancers, version 2.2025, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw 2025;23:403–18.

{kind=link}
{kind=link}