





Abstract
Laparoscopic transabdominal preperitoneal (TAPP) repair is the gold standard for treatment of inguinal hernia. Its complications are well known; however, its rare complications, such as mesh erosion and migration are commonly overlooked. There is established evidence about mesh complications; however, we have not found a similar case to what we encountered. We present a case of an elderly male who presented with a closed-loop bowel obstruction following a TAPP repair. Intraoperatively, the appendix tip was adherent to the eroded mesh through a defect in the peritoneal flap. The appendix formed a constricting wrap around the terminal ileum with a resultant ischemia of the bowel in the presence of a competent ileocecal valve. Reasons accounting to mesh erosion can be divided into primary and secondary causes. Complications from mesh erosion vary from fistulation up to bowel ischemia. Failure to recognize these complications can lead to considerable morbidity.
Introduction
Laparoscopic hernia repair with mesh is becoming widely accepted as the gold standard for elective treatment of inguinal hernias [1]. Reasons for choosing laparoscopy over open repair are well known and include shorter hospital stay, better healing, less pain, and faster recovery. Complications post laparoscopic inguinal hernia repair are well known, however, rare complications such mesh erosion after surgery and the subsequent sequela of the erosion are seldom investigated [2]. While there are some cases reported in literature describing complications from mesh erosion, such as adhesional small bowel obstruction, adhesion into the urinary bladder causing fistulas, and large bowel obstruction resulting in ischemia, we have yet, to our knowledge, to see a similar case to what we have encountered [1, 2, 3]. We present a case of a 76 year old male who presented with high grade closed loop small bowel obstruction due to the erosion of mesh and subsequent attachment to the appendix tip causing the appendix to wrap around the terminal ileum in the presence of a competent ileocecal valve.
Case description
We present a case of a 76-year-old gentleman who had a previous elective laparoscopic TAPP right inguinal hernia repair in another hospital on January 2023. The procedure reportedly went well with no complications. The patient then presented on March 2023, 2 months after his procedure, with symptoms of small bowel obstruction. The initial computed tomography (CT) scan showed high-grade small bowel obstruction (Figs 1 and 2). The patient was initially treated conservatively as for most cases of small bowel obstruction thought to be attributed to adhesions from recent surgeries. The decision was made to take the patient for a diagnostic laparoscopy 48 hours after conservative management failed to resolve symptoms. Laparoscopically, gross small bowel ischemia was noted, and a tube-like structure was seen wrapping around the ischemic segment (Figs 3 and 4). The decision was taken to convert the procedure to an open one due to massive bowel dilatation and the inability to define the nature of this adhesive wrap. Upon conversion, it was noted that this tube-like structure causing the band was indeed the appendix wrapping around the terminal ileum, with its distal part adhered to the eroded mesh from the peritoneal flap of the recent TAPP repair. The decision was taken to perform a limited ileocecal resection and primary anastomosis. The protruding part of the mesh was excised, and the appendix resected. The peritoneal flap was closed with sutures. The patient did very well postoperatively and was discharged a couple of days later.

Transverse cross sectional view of mottled small bowel in the pelvis as a result of the closed loop obstruction.

CT image showing a sagittal cross-sectional view of the affected SB loops.
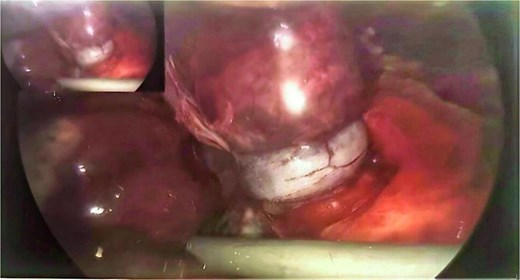
Operative image showing appendix wrapped around and constricting the terminal ileum (taken with permission).

Operative image showing a panoramic view of the closed loop obstruction causing small bowel ischemia (taken with permission)
Discussion
Laparoscopic elective inguinal hernia repair is a relatively safe operation with low rates of complications. Less commonly occurring complications in literature include trocar injury, injury to major vessels, injury to urinary bladder and intestine, and mesh erosion or migration [1]. While small bowel obstruction (SBO) is a known but relatively rare complication following elective laparoscopic inguinal hernia repair, with rates ranging between 0.2% and 0.5%, it can variably be attributed to different causes [4]. Mesh erosion in itself can cause small bowel obstruction [1]. More rarely is the case in which small bowel obstruction resulting from the mesh erosion will cause bowel ischemia. While there are cases in the literature describing bowel ischemia from mesh erosion [5], we have yet to see, to our knowledge, a case of small obstruction due to mesh erosion causing the appendix to wrap around the terminal ileum, resulting in closed-loop obstruction and small bowel ischemia in the presence of a competent ileocecal valve.
Mesh erosion should always be considered in cases of small bowel obstruction following elective laparoscopic inguinal hernia repair, along with the more common causes of obstruction. Initially, the patient should be treated as any case of SBO with bowel rest, nasogastric tube, intravenous fluids, input and output charts, urinary catheter and periodic review of progression of symptoms. This is, of course, in the hemodynamically stable patient. The decision to operate will depend on the failure of resolution of obstruction following the conservative management period and the high clinical sense for the progress of management. Causes of mesh erosion have been mainly attributed to mesh infection or peritoneal damage. Inadequate closure of the peritoneal flap can easily lead to this rare complication as well [1]. Agrawal and Avill [6] have cited the attribution of mesh migration due to primary and secondary causes. Primary mechanical migration of the mesh is caused by displacement of the mesh along the path of least resistance and can be caused by inadequate fixation or external displacing forces. Secondary causes can be attributed to foreign body reactions caused by the type of mesh, infection, and poor healing mechanisms. The sharp cuts of the mesh can also lead to it being eroded outside of the peritoneal flap, causing complications [7].
Conclusion
Mesh erosion and migration can cause considerable morbidity following elective laparoscopic inguinal hernia repair. Of these complications, small bowel obstruction is a serious one with rare occurrences. Operative management is usually required when the organ adheres to the eroded mesh causes SBO. Consideration should always be given to prevent primary and secondary causes of mesh erosions/migration. Failure to do so can lead to post-operative catastrophes.
Conflict of interest statement
None declared.
Funding
None declared.
Patient consent
Written informed consent was obtained.

{kind=link}
{kind=link}
{kind=link}
{kind=link}