





Abstract
Diverticular diseases uncommonly occur at a young age. However, its prevalence in younger individuals is rising. Atypical presentations will lead to misdiagnoses and unindicated surgery. Colovesical fistulas remain the most common type that is associated with diverticular diseases. A 16-year-old female patient presents with 2 months history of left-sided lower abdominal pain, in addition to, longstanding history of urinary incontinence since early childhood. Imaging studies, including computed tomography and magnetic resonance imaging, revealed complicated sigmoid diverticulitis by fistula formation to the urinary bladder and uterus, possible fistula to the vagina and rectum. The patient underwent successful surgical intervention, including sigmoidectomy, closure down of the colovesical fistula, and keeping of the vesicouterine fistula with plans for future repair by a specialized urogynecologist.
Introduction
Diverticular diseases uncommonly occur at a young age in which <10% of people under the age of 40 were reported cases [1]. Well-known risk factors include obesity, low fiber diet, sedentary lifestyle, and old age [2–4]. Diverticulitis remains the most common complication of diverticulosis at the rate of 10%–25% [1, 5]. Atypical presentation will lead to misdiagnoses and unindicated surgery [2]. Colovesical fistulas remain the most common type that is associated with diverticular diseases [6]. This case report presents a rare occurrence of complicated sigmoid diverticulitis in a 16-year-old female, complicated by colovesical and vesicouterine fistulae with a suspicion of the presence of vesicovaginal and vesicorectal fistulae.
Case presentation
A 16-year-old female with history of developmental delay was referred to our hospital for management of complicated diverticulitis with abscesses formation. The patient reported 2 months history of left-sided lower abdominal pain, weight loss, and reduced oral intake. In addition, longstanding history of urinary incontinence since early childhood, which left her dependent on diapers. On physical examination the patient was afebrile, with normal vital signs, she has a short stature, with abnormal fascial features and abnormal teeth, and she has long fingers with small hands. Her abdomen was soft and non-tender. The remaining of the physical examination was unremarkable. Investigations at admission showed anemia and elevated C-reactive protein. Other parameters, including white blood cell count and electrolytes, were within normal limits.
Computed tomography (CT) abdomen and pelvis showed perforated sigmoid diverticulitis, extraluminal collection measuring 3 × 1.8 cm, fistula formation extending to left aspect of urinary bladder dome, and another fistula possibly extending to anterior wall of rectum (Fig. 1).
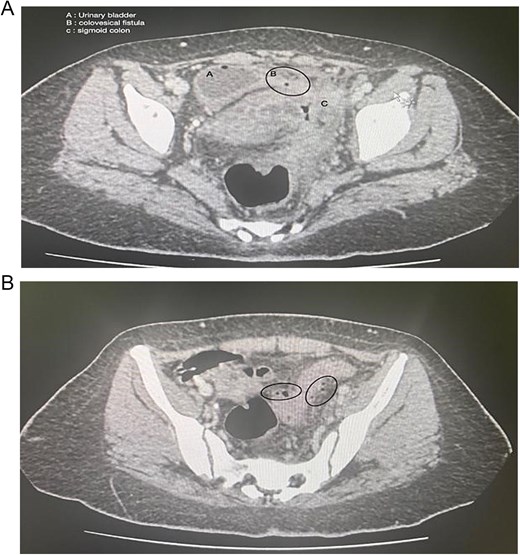
(A) Axial section of the abdominopelvic CT scan showing the colovesical fistula. (B) Axial section of the abdominopelvic CT scan showing the diverticular disease of the colon.
Colonoscopy showed severe luminal narrowing between the junction of the sigmoid and descending colon. Diagnostic cystoscopy confirmed the presence of a fistula opening and demonstrated a villous-like reaction in the urinary bladder mucosa, consistent with a fistulous connection. The fistula opening was located low, raising the possibility of vesicovaginal fistula. Magnetic resonance imaging (MRI) of the abdomen conformed sigmoid diverticulitis and fistula tract to urinary bladder and also possibly a fistula tract extending to the mid-rectum (Fig. 2).
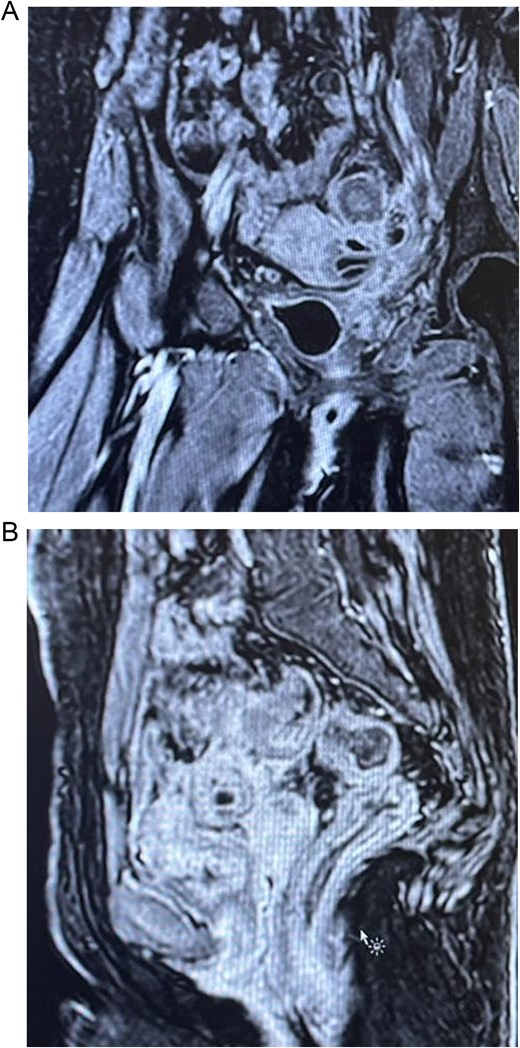
MRI scan.
The patient was admitted and started on intravenous hydration and antibiotics. She was kept nothing-by-mouth in preparation for surgery. Mother consented for laparoscopic sigmoidectomy, with an anastomosis versus end colostomy creation, with possible partial cystectomy, left oophorectomy, and bilateral prophylactic ureteric catheter or stent, colleagues from urology were informed about possible intraoperative needs, preoperative stoma marking was done.
The patient underwent the surgery, intraoperative findings revealed inflamed sigmoid colon, extensive fibrosis, and a stony-hard adhesion between the sigmoid and left lower abdominal wall. A fistula between the sigmoid and urinary bladder was identified and released with primary closure of the defect (Fig. 3). Another fistula was discovered between the left side of the uterine fundus and the urinary bladder, characterized by wide diameter and dense adhesions. Urology and gynecology consultants were involved in intraoperative decision-making. After thorough discussion, it was concluded that excision of the vesicouterine fistula at this stage would result in significant defects in both organs, requiring major reconstruction. Therefore, the repair of the vesicouterine fistula was planned for a later stage by a urogynecologist.
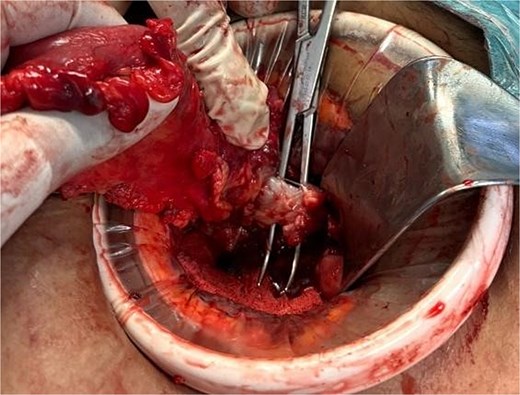
Intraoperative finding of the colovesical fistula.
A sigmoidectomy was done, followed by an end to side colorectal anastomosis, with no intraoperative complications. The patient showed significant improvement in her symptoms after surgery by resolving her abdominal pain and urinary symptoms. Follow-up CT cystogram was done, which was unremarkable with no clear vesicorectal or vesicovaginal fistula (Fig. 4). Histopathology was performed and confirmed the presence of diverticular disease with chronic mucosal changes and fibrous tissue consistent with fistula formation, in addition to, the absence of histological evidence of dysplasia, or malignancy.
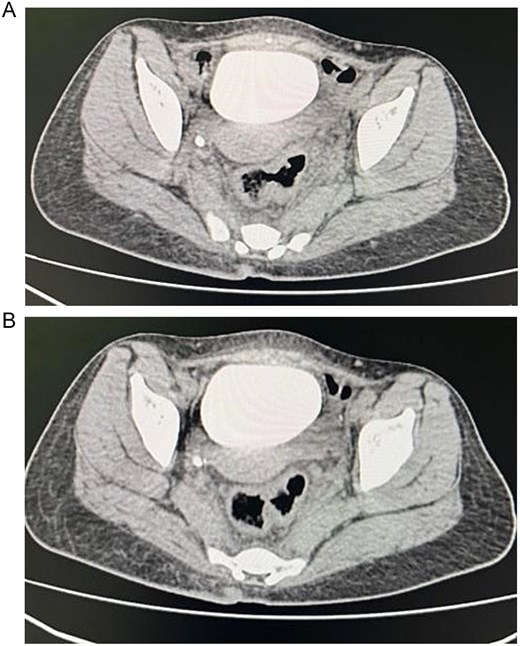
Showing axial section of the abdominopelvic CT scan with cystogram showing contrast filled urinary bladder with no clear vesicorectal or vesicovaginal fistula.
Discussion
Diverticular disease traditionally occurs in elderly adults, new evidence suggests occurrence in younger populations [1, 7]. While the condition is still rare in this age group, it appears to occur in young males and individuals with obesity [2]. In our case, a 16-year-old female with no typical risk factors for diverticulitis, such as age, constipation, and obesity, presented with complicated sigmoid diverticulitis complicated by colovesical and vesicouterine fistulae.
Studies have suggested that diverticulitis in younger patients may present with an aggressive course compared to that in adults [3, 4]. In our case, the patient’s young age did not directly correlate with her severe presentation, but the presence of multiple fistulae, adhesions, and abscess formation indicated surgical intervention. This case emphasizes the vitality of formulating an individualized approach in management based on the disease severity and outcomes.
Colovesical fistulae remain the most common type that is associated with diverticular disease [6]. On the contrary, vesicouterine fistulae are rare in the context of diverticulitis and rarely described in literature. To date, there have been no documented association between vesicouterine fistulas and diverticulitis, making this case potentially the first to suggest a correlation between these two clinical entities. While it is possible that the patient’s history of developmental delay, urinary incontinence, and intellectual disability may indicate a congenital etiology for the vesicouterine fistula, this should be investigated further in future studies.
The approach to intervention whether medical or surgical in the case of diverticulitis in young patients remains contentious, relying on the severity of the disease and its presentation [8, 9]. In our case, surgical intervention was necessary due to disease severity. The patient underwent successful surgical intervention, with resection and end-to-side colorectal anastomosis, with no postoperative complications. On the subsequent outpatient visits, we offered a referral to a urogynecologist, but the patient and mother were satisfied with the outcome and that a dramatic improvement was noticed. This approach that was taken with the patient is consistent with modern, evidence-based guidelines advocating stage management in adults. This raises the urgent need to study and formulate an up-to-date guideline on the approach to managing a case of diverticulitis within this young age group.
Conflict of interest statement
The authors declare no conflicts of interest.
Funding
No funding was received for this study.
Ethical approval
Ethical approval was not required for this case report. Written informed consent was obtained from the patient for publication.
Consent
Written informed consent was obtained from the patient for the publication of this case report and accompanying images.

{kind=link}
{kind=link}
{kind=link}
{kind=link}