





Abstract
Foreign body ingestion is a common problem in pediatrics; some of them can be life-threatening, such as button batteries, magnets, and sharp, pointy objects. Due to the intestine's intrinsic capacity to protect against these events, most foreign bodies pass without harm. Nonetheless, severe complications can arise in some patients. Therefore, prevention, parent education, a high index of suspicion, and close surveillance are essential tools to treat these patients. We present the case of a toddler who accidentally ingested a foreign body (key) and was placed under close surveillance since she was asymptomatic. After 72 hours the key passed and she fully recovered.
Introduction
Foreign body ingestion is a frequent problem in pediatrics (up to 70% of cases occur in children under 4 years of age) [1, 2]. It is essential to monitor children closely and never leave them unattended to prevent these situations [2]. Most ingested foreign bodies will pass through the gastrointestinal tract spontaneously and without complications, but high awareness is necessary to avoid complications [1, 3].
We present the case of a 6-year-old female who accidentally ingested a key while playing. She did not suffer any pain or complications, and the key passed through her gastrointestinal tract without complications.
Case report
The patient is a 6-year-old female without past medical history. While playing with her older brother, she found some keys and started to play with them. She put one key in her mouth and inadvertently swallowed it. The two kids hid what had happened, fearing their mother would punish them.
However, after 1 day, the girl became more anxious and frightened and told her mother everything that had happened. After her mother learned about it, she quickly took her to the emergency room. It should be mentioned that the patient remained asymptomatic during all this time.
On clinical evaluation, a completely asymptomatic patient was encountered; she was extremely nervous. However, her vital signs were normal, and she had no abdominal pain or tenderness. She passed gas and had no issues with her bowel movements. Due to this, an abdominal X-ray was requested, unveiling a foreign body (small key) in her abdomen. The foreign body appeared to be in her stomach or transverse colon; nonetheless, it did not cause any signs of obstruction (Fig. 1a and b). With these findings, the patient was admitted for close monitoring due to the risk of obstruction. An endoscopy was requested. However, it was completely normal, and the key was nowhere to be found as it had already passed through the pylorus. Another abdominal X-ray was done 48 hours after admission, showing that the foreign body was moving along the intestines (Fig. 2).
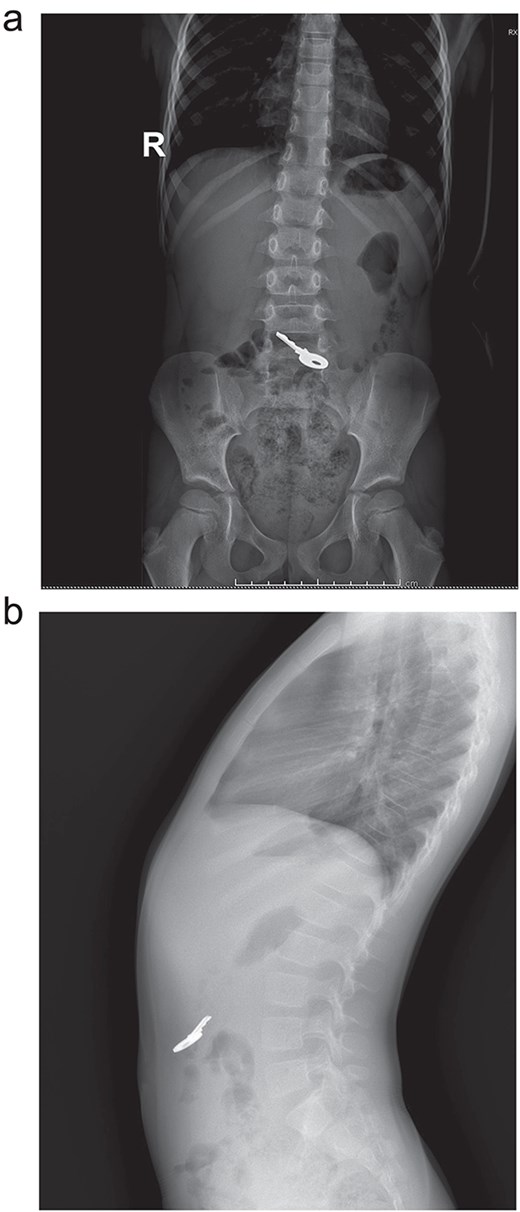
(a) X-ray: A full key is seen ingested, no pneumoperitoneum or signs of obstruction. (b) X-ray: the key is seen in the intestine.

X-ray: the key is seen moving and changing position.
After seventy-two hours in the hospital and after close surveillance, the foreign body (key) was expelled with feces without any complications. The kid was discharged, and dietary and care-taking recommendations were given to the parents.
On follow-ups, the patient is doing well without complications.
Discussion
Foreign body ingestion is a common situation that tends to occur as an accident in children between 6 months and 3 years of age [1, 2]. Nonetheless, any person can be affected, even adults (psychiatric disorders or suicidal thoughts) [1, 3]. Fortunately, most foreign bodies will pass through the gastrointestinal tract without complications [1]. Less than 10% to 20% of foreign bodies must be removed through endoscopy, and <1% will need surgery [1, 2].
Several locations of the gastrointestinal tract can make it difficult for foreign bodies to pass through; therefore, it can cause obstruction, perforation, bleeding, and other complications (adhesions, malformations, neuromuscular illness, pylorus, stomach, duodenum, ileocecal valve, and Meckel's diverticulum) [1, 4].
Symptoms will depend on the location of the foreign body [2, 5]. If it is trapped in the esophagus, children may experience a sore throat or difficulty swallowing [3, 4]. If it's in the stomach, many patients will be completely asymptomatic or present with abdominal pain, vomits, and nausea and may refuse meals [4, 5]. If the foreign body passes into the small bowel, it will most likely pass spontaneously with bowel movements; however, it can cause abdominal pain and bloody stools [2, 6]. Therefore, strict surveillance must be done due to the risk of perforation and complications [1, 6]. Signs and symptoms of ingestion are not usually perceptible, as most cases happen when children are alone without supervision [1, 2]. Therefore, many foreign bodies can be missed or discovered incidentally on a chest or abdominal X-ray for non-specific symptoms [2, 3].
In our case, the patient was afraid of her mother because she knew what she had done was wrong; however, even though it was late, she told her mother everything.
Once a diagnosis is made, an endoscopy should be performed quickly to remove the foreign body [1, 4].
Thanks to the developments in technology and awareness of endoscopy in children, it has proven to be extremely useful; however, one must consider the children's age, weight, presentation, time since the last meal, and the size and shape of the foreign body. [4, 6] The foreign body can also be observed over 12–24 hours if the child is asymptomatic and has no history of previous surgery, as >60% of foreign bodies less than 25 mm can pass spontaneously [1, 3, 7]. Imaging with X-rays or computed tomography will be needed to confirm the presence and location of the foreign body inside the intestine [6, 7].
In our case, the patient was always asymptomatic. Since the foreign body appeared in the stomach on the first X-ray, we decided to perform an endoscopy, which proved ineffective. After an adequate waiting period, the key came out without complications.
The nature and shape of an ingested foreign body are essential, as many can cause severe damage if left untreated [1, 5]. Batteries can cause severe damage due to hydrolysis and cause caustic injuries within 4 hours of ingestion; therefore, they should be removed in <2 hours [3, 4]. Coins can be observed depending on their size and location; magnets can attract each other and cause fistulas and severe complications; therefore, they should be removed as fast as possible [1, 7]. Pointed and sharp foreign bodies are especially at risk of causing perforation, and this risk rises dramatically (15% to 35%) [2, 3].
Early diagnosis and timely treatment are key to avoiding complications; these should always be accompanied by prevention and parent education campaigns.
Conclusion
Even though the prognosis for ingested foreign bodies is usually good, strategies to prevent children from being in contact with small toys, keys, remote controllers, or batteries are and will always be the best treatment. Preventing these potential dangers and complications is and will always be our greatest tool. Remembering never to leave children unattended.
Conflict of interest statement
None declared.
Funding
None declared.

{kind=link}
{kind=link}