





Abstract
Dedifferentiated liposarcoma (DDL) is an aggressive subtype of liposarcoma that rarely arises within the abdominal cavity. We describe the case of a 71-year-old female incidental transverse colon mass suspicious for colorectal cancer. Pre-operative biopsy at colonoscopy was not possible due to the lesion’s extraluminal location; however, complete resection was achieved through left hemicolectomy. Histology confirmed DDL. Review of the literature found four additional cases of DDL in the transverse colon. Clinical presentation, management, and follow-up were reviewed, illustrating poor outcomes; three of the five cases died within 3 years of surgery. DDL is associated with higher rates of local recurrence, metastasis, and mortality compared to well-differentiated liposarcomas. While limited by its rarity, DDL in the transverse colon appears to follow similarly poor outcomes.
Introduction
Liposarcomas are the commonest soft tissue sarcoma, with five histological subtypes: well-differentiated liposarcoma (WDL), dedifferentiated liposarcoma (DDL), pleomorphic, myxoid, and round cell [1, 2]. WDL and DDL constitute the largest subgroup of liposarcomas [2], representing a continuum of the same disease process [3]. DDL is more aggressive in its behaviour; it has capacity for metastasis where WDL does not and a greater propensity for local recurrence [3]. Typically, DDL is found most frequently in the retroperitoneum but can also be found in the extremities, paratesticular area, and head and neck [3]. It is rarely found within the abdominal cavity [4]. Here, we present a rare case of DDL in the transverse colon.
Case report
A 71-year-old female presented with a 6-week history of intermittent lower abdominal pain and subjective fevers and altered bowel habit without any obstructive symptoms or gastrointestinal bleeding. She had a history of well-controlled hypertension, chronic kidney disease, and smoking. Examination revealed lower abdomen tenderness with no palpable masses.
CT abdomen and pelvis was showed uncomplicated diverticulitis; however, a lobulated 54 × 54 mm exophytic mass arising from the transverse colon with adjacent enlarged lymph nodes was incidentally noted (Figs 1 and 2). Colonoscopy, limited by diverticulosis, found no intraluminal mass but revealed desmoplastic mucosal changes at the splenic flexure. Biopsies were nondiagnostic. Staging CT chest showed no metastases, and CEA was 4.0.

CT abomen + pelvis with contrast demonstrating ~5 × 5 cm exophytic lobulated mass at splenic flexure, appearing to arise from transverse colon.
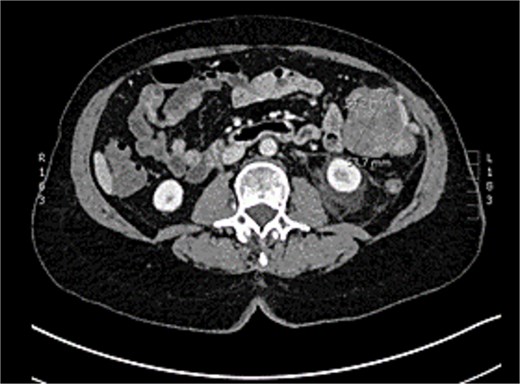
CT abomen + pelvis with contrast demonstrating ~5 × 5 cm exophytic lobulated mass at splenic flexure, appearing to arise from transverse colon.
She was discussed at the colorectal radiology multidisciplinary meeting; surgical resection was recommended. A laparoscopic-assisted left hemi-colectomy was performed. A large exophytic transverse colon lobulated lesion was identified. The inferior mesenteric vein and left colic artery (preserving distal sigmoid branches) were ligated, and an end-to-end hand sewn anastomosis between distal sigmoid and mid transverse colon was created. Tumour capsule integrity was maintained.
Postoperative complications included an anastomotic leak on day 5, requiring laparotomy, repair and diverting ileostomy. Unfortunately, the patient subsequently developed a 6 × 10 cm anterior abdominal wall collection drained by interventional radiology, which cultured Pseudomonas aeruginosa and Enterococcus faecalis. After prolonged intravenous antibiotics, the patient made a full recovery and was discharged 1 month after her initial operation.
Histology revealed a multilobulated spindle cell lesion, with low- and high-grade areas, with an abrupt transition between these areas. There was an adjacent focus of adipose tissue with rare cytologic atypia suggestive of possible WDL, which indicated that the tumor mass may represent DDL. However, there was a single focus of lipoblasts identified, bringing up the differential of pleomorphic liposarcoma. Therefore, in situ hybridisation was performed and showed MDM2 amplification, which confirmed the diagnosis of DDL, with likely homologous lipoblastic morphology. The tumour was excised with clear margins (Figs 3–8).
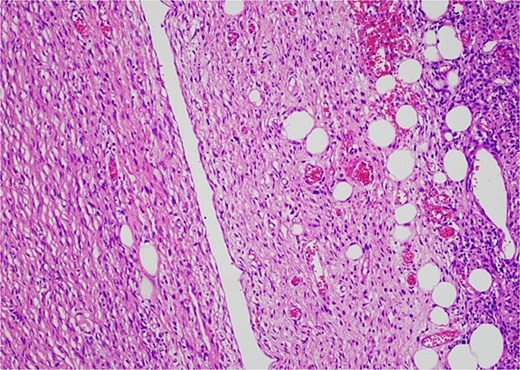
Low-grade component with spindle cells with tapered nuclei and indistinct cytoplasm that merges into a delicate collagenous stroma.
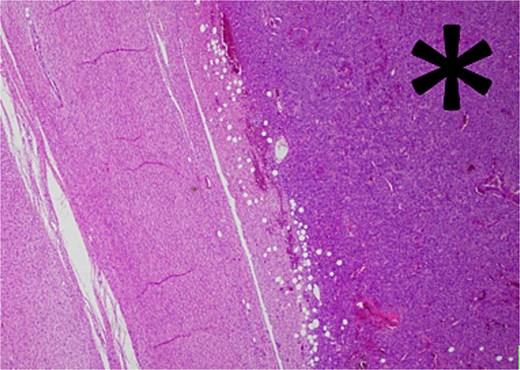
Low-grade component with abrupt transition to high-grade component (asterisk).
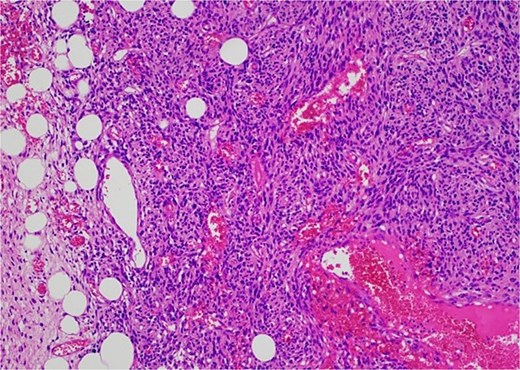
The high-grade component demonstrates increased cellularity, hyperchromasia and moderate to marked pleomorphism including scattered multinucleate cells.
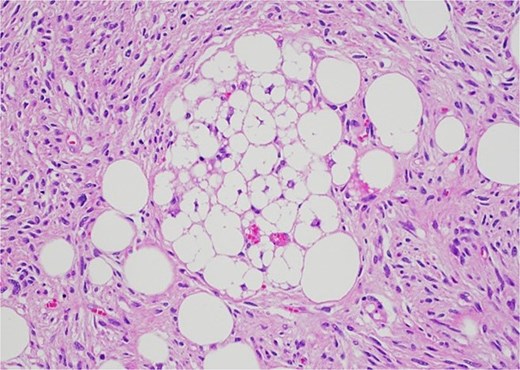
The lesion contained a single of lipoblasts.

Macroscopic pictures of resected transverse colon with tumour.
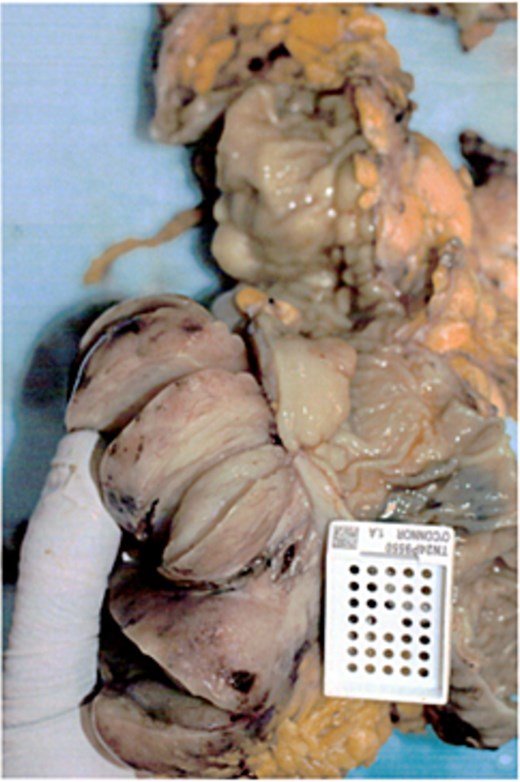
Macroscopic pictures of resected transverse colon with tumour.
The case was discussed at the state-based sarcoma multidisciplinary meeting, recommending no further treatment and serial imaging surveillance.
Discussion
Primary DDL arising from the colon is an exceptionally rare presentation of an already uncommon disease. A literature review of colonic liposarcoma in 2020 found only 28 case reports describing primary colonic liposarcoma, of which four cases were the DDL subtype [4]. Only one of these primary colonic liposarcomas was reported to have arisen from transverse colon [5]. Further review of the literature found three other cases of primary liposarcoma arising from the transverse colon; of interest, all four of these cases were the DDL subtype as in this current case presentation (Table 1) [5–8].
Literature review of cases dedifferentiated liposarcoma of transverse colon.
| Authors | Presentation | Location | Surgery | Adjuvant treatment | Follow-up |
|---|---|---|---|---|---|
| Turkoglu 2014 [5] | 71-year-old female abdominal pain, and intraabdominal mass | Arising transverse colon, invading stomach | Laparotomy + segmental colon and gastric wedge resection | Radiotherapy planned but patient declined | Widespread metastatic disease and patient died within 3 months of surgery |
| D’Annibale 2009 [6] | 79-year-old female abdominal pain, progressive constipation, and weight loss | Transverse colon focus with multiple other intra-abdominal deposits | Laparotomy + right hemicolectomy + partial gastric resection + excision of the omental and mesocolic masses | Radiotherapy | 28 months after surgery developed progressive dysphagia and radiological evidence tumour progression 30 months after surgery died after an acute cardiac event |
| Fitzgerald 2022 [7] | 66-year-old female abdominal pain with rectal bleeding | Transverse colon | Robotic segmental colectomy | No adjuvant treatment (clear margins + nil nodal involvement/distal metastasis) | 1-year follow-up, disease-free |
| Kuroda 2022 [8] | 70-year-old female right lower abdominal mass | Transverse colon + abutting mesentery | Intrabadominal mass resection + partial resection of transverse colon + biopsy small bowel mesentery | Adjuvant chemotherapy | 18 months after surgery patient died due to perforation bowel lesion |
| Current Case | 71-year-old female abdominal pain and fevers | Transverse colon | Laparoscopic left hemicolectomy | No adjuvant treatment (clear margins + nil distal metastasis) | 3 months follow-up, disease free |
DDL typically presents in middle-aged to older adults and can be asymptomatic or manifest as abdominal pain, a palpable mass, gastrointestinal bleeding, or mechanical obstruction of the bowel or urinary system [3, 4] which was consistent with presentations in transverse colonic DDL. Pathognomic finding of DDL on CT or MRI is a heterogeneous, nonlipogenic encapsulated mass [9].
DDL most commonly has the histological appearance of undifferentiated pleomorphic or spindle cell sarcoma; however, various morphological presentations which can make diagnosis difficult. However, DDL is associated with high levels of amplifications in chromosome 12; in particular, the CDK4 and MDM2 cell cycle onocogenes. As in this case, fluorescence in situ hybridisation testing to assess for MDM2 gene amplification can be a useful diagnostic tool to help distinguish DDL from sarcomatous mimics [3].
Surgical resection is the mainstay of treatment of DDL [3]. While adjuvant chemoradiotherapy is not curative, it may have a role in the management of advanced disease or delaying progression in select patients [10]. Systemic treatments for DDL are rapidly evolving, with evidence that novel agents may have a clinical benefit in recurrent or metastatic disease. In particular, targeted therapies exploiting the fact that nearly all DDL include highly amplified expression of MDM2 and CDK4 are in development [11].
Generally DDL is one of the more aggressive subtypes of liposarcoma with a five-year and 10-year survival rate of 57.2% and 40.1% respectively compared to WDL with survival rates of 100% and 82.1% [12]. Apart from DDL histological subtype, other statistically significant negative prognostic factors for patients with liposarcoma include larger tumour size, local recurrence, metastatic disease, incomplete resection, and older age [13, 14].
DDL has an estimated local recurrence rate of 40%, metastatic rate of 17% and disease-related mortality rate of 28% generally [15]. Local recurrence of any liposarcoma significantly lowers survival rates in the long term (5- and 10-year survival rates of 86.2% and 49.0%, respectively, compared with 86.7% and 82.9% without). Metastases of liposarcomas have been demonstrated in bone, lungs, soft tissues, and lymph nodes. Five and 10-year survival in patients without metastases has been reported at 96.8% and 93%, respectively, compared with 45.6% and 21.9% with metastatic disease [12]. Due to its rarity, specific rates of colonic recurrence are unknown; however, from the review of cases of DDL in transverse colon outcomes, they are generally very poor (Table 1).
In conclusion, primary colonic DDL is rare, with only five cases involving the transverse colon, including this current case presentation. Our findings further support that DDL is an aggressive tumour with relatively poor prognosis. Ongoing research is required to further categorise its clinical characteristics and develop further therapeutic options, particularly in cases of local recurrence or metastatic disease.
Acknowledgements
Thank you to Dr Jason Pimental for his expert pathology review.
Conflict of interest statement
None declared.
Funding
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}