





Abstract
The success of hemisection is based on meticulous case selection, considering the quality and quantity of bone surrounding the remaining roots. Additionally, a well-devised prosthetic plan is crucial to direct forces along the preserved roots, and ongoing maintenance is imperative for long-term success. This case report aims to present two different restorative designs for the pontic on the edentulous space after the hemisection of a molar tooth. The treatment approach included initial root canal treatment, followed by periodontal intervention involving hemisection. The hemisected tooth was restored through a fixed partial denture, utilizing premolar, or molar as abutments. Hemisection is an excellent option for retaining the molar tooth in the mouth. The restorative option might be chosen between original molar anatomy or transformation into premolars. This must be in accordance with the patient’s wishes as well.
Introduction
Restorative dentistry aims to preserve the natural dentition, ensuring the patient’s comfort while restoring the dentition based on evidence-based dentistry. To achieve this, the retention of the roots or part of the root in the multi-rooted tooth is very crucial to support the coronal restoration, either full coverage indirect restoration, fixed partial denture (FPD) restoration, or removal of partial dentures.
Caries more frequently affect the first molar tooth, which can lead to premature extraction of the tooth [1, 2]. Molar teeth play a crucial role in maintaining proper occlusion and maintaining adequate function of chewing for patients [3]. They have the capacity to withstand forces up to 20 000 Mpa during the chewing process [4]. However, the anatomy of the molar teeth can be problematic once pathological disease occurs, for example, localized periodontal disease with significant bone loss or periapical disease with significant periapical pathology, which may compromise one of the roots in these molars.
Regardless of these shortcomings, part of the root may be able to provide adequate retention and support to retain the coronal restorations (Single crown, FPD, or RPD). Molar root hemisection is a technique where the poor prognosis root is removed while maintaining the good prognosis ones in a multirooted tooth after completion of the root canal treatment or stabilization of the periodontal disease [5]. The remaining root can either be a crown or serve as an abutment for FPD or RPD. Hemisection is a biological and cost-effective procedure, yielding favorable long-term results [6] while maintaining the natural occlusion. This is essential for proper function and preventing issues related to pathologic tooth migration or misalignment, perhaps considering the potential for hemisection should precede the decision to extract any molar tooth [7].
This case series will report on hemisection cases performed on mandibular molars in patients with deep root caries. These cases present two different prosthetic design approaches in restoring the hemisected mandibular root.
Clinical case 1
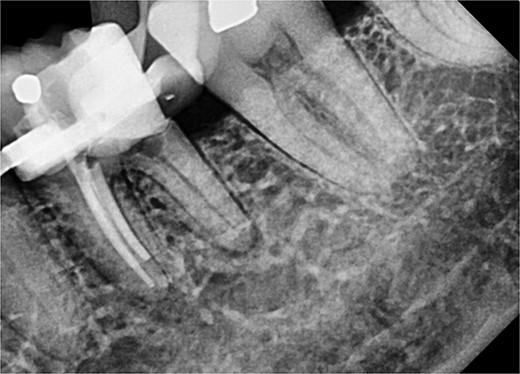
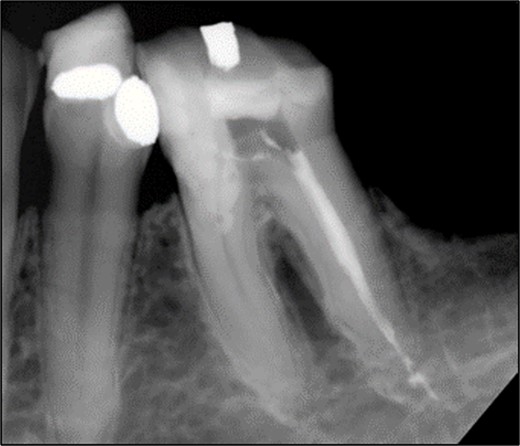
A 44-year-old patient presented to our clinic with the primary complaint of food lodgment in a cavity on the lower left posterior teeth. Clinical examination revealed extensive caries on the disto-occlusal surface of the lower left first permanent molar (tooth 36) (Fig. 1). Radiographic examination showed a large radiolucency at the distal crown extending to the cervical third of the distal root, with periapical radiolucencies on both mesial and distal roots (Fig. 2). The tooth was diagnosed with asymptomatic irreversible pulpitis and symptomatic apical periodontitis.

Clinical photograph of tooth 36 showing extensive caries on disto-occlusal surface.

Periapical radiograph of tooth 36 showing a large radiolucency area at the distal crown involving the cervical third of the distal root.
Non-surgical root canal treatment was initiated under local anesthesia and rubber dam isolation. Pulp extirpation was performed on all canals (mesio-buccal (MB), mesio-lingual (ML), and distal (D)). The MB and ML canals were instrumented using ProTaper Gold files and obturated with a bioceramic sealer (iRoot SP). The orifices were sealed with glass ionomer cement (Fuji IX) (Fig. 3).
Periapical radiograph of tooth 36 with obturation on MB and ML canals.
Following root canal treatment, hemisection and removal of the distal root were performed under local anesthesia. The furcation area was marked on the crown to guide tooth sectioning. Using a low-speed surgical fissure bur under normal saline irrigation, a vertical cut was made to separate the tooth. The distal root was elevated and removed in one piece using a periosteal elevator. Sharp edges and margins were smoothened, and the coronal tooth structure was restored. Hemostasis was achieved using a pressure pack.
The patient was monitored for one year with no reported symptoms. Due to extensive filling and secondary caries in the adjacent left second mandibular molar (tooth 37), both the mesial root of tooth 36 and tooth 37 were prepared for a zirconia bridge. Tooth 36 received a full-coverage crown, while tooth 37 was restored with an onlay. Tooth 36 was anatomically restored to conform esthetically and functionally with the existing occlusion (Fig. 4 and 5).
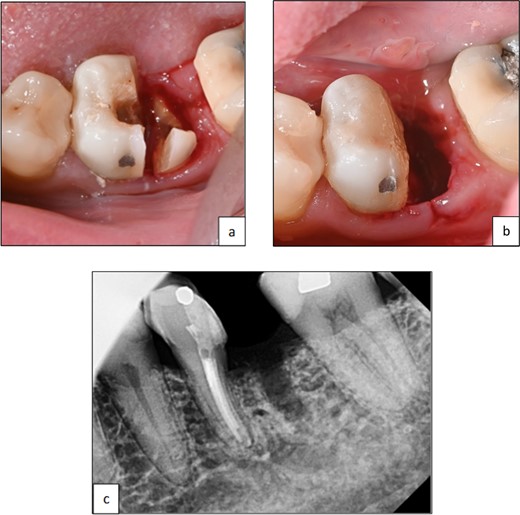
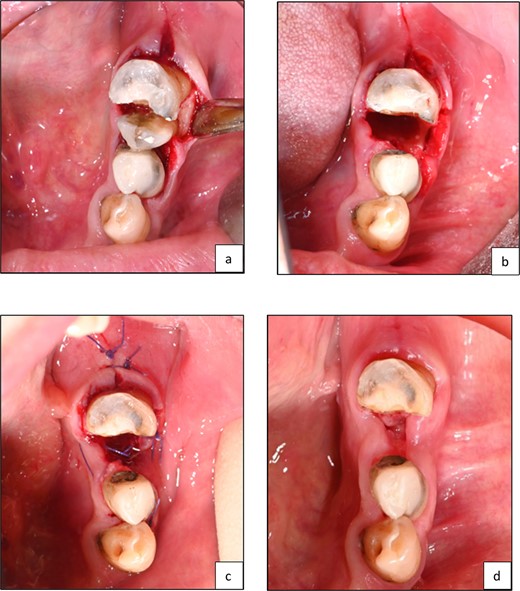
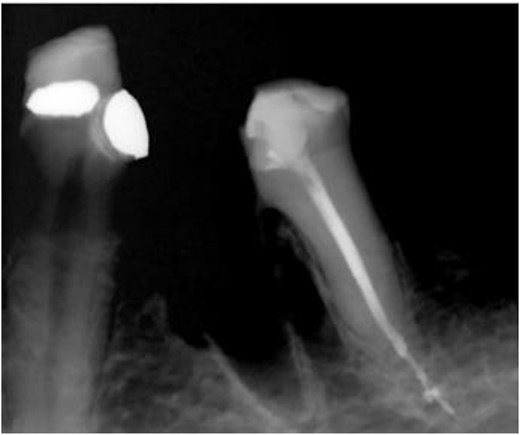
Clinical photographs showing (a) line of resection through furcation area and separation of mesial and distal roots, (b) after elevation of root and smoothening of sharp edges, (c) periapical radiograph of tooth 36 after hemisection and removal of distal root.
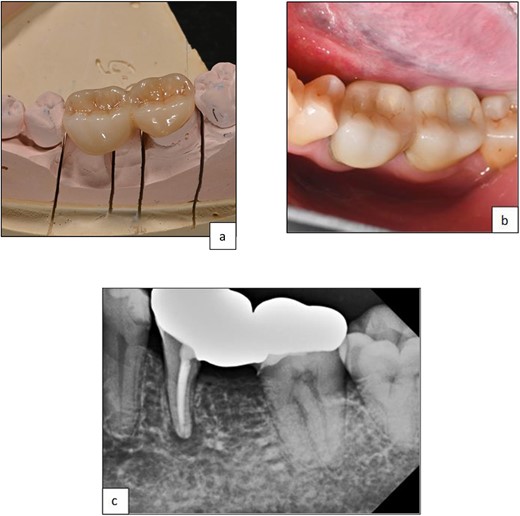
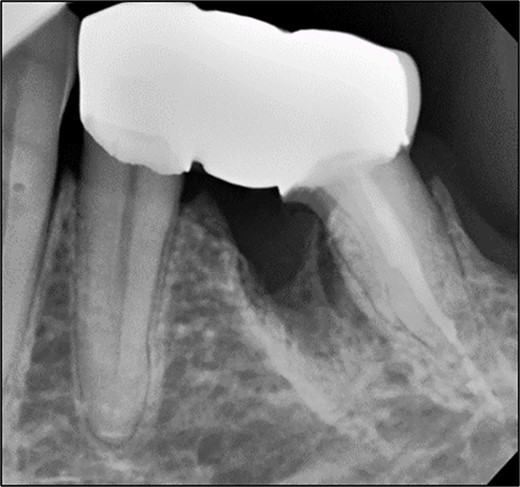
Clinical photographs showing (a) zirconia bridge design, (b) final prosthesis after cementation, (c) periapical radiograph post-cementation of zirconia, the bridge shows a good adaptation of the restorative margins.
Clinical case 2
A 59-year-old male patient presented with a complaint of pain while biting on his lower left posterior teeth. Clinical examination revealed an extensive amalgam restoration on the lower left first molar (tooth 36) with a fractured restoration and secondary caries on the lingual aspect. The tooth was non-responsive to thermal testing and electrical pulp sensibility testing (EPT) and was tender to percussion. Radiographic examination showed radiolucency beneath the restoration on the mesial root surface, indicative of caries, along with furcation involvement and peri-radicular radiolucency. The tooth was diagnosed with pulpal necrosis and symptomatic apical periodontitis associated with extensive root caries (Fig. 6 and 7).
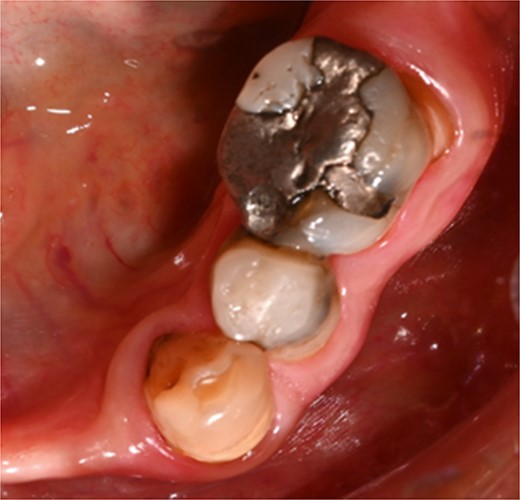
Clinical photograph of tooth 36 showing extensive amalgam restoration on mesio-occlusal-disto-bucco-lingual (MODBL).

Periapical radiograph of tooth 36 shows large radiopacity, indicating a restoration on the crown extending to the mesial root surface. Radiolucency was detected beneath restoration on the mesial root surface, indicating caries. Peri-radicular radiolucency was observed in the furcation region.
After removal of the existing restoration and caries, the cavity margin on the mesial side was noted to be 1 mm subgingival, with a mid-palatal margin extending to the root surface. Non-surgical root canal treatment was performed under local anesthesia and rubber dam isolation. Only the DB and DL canals were cleaned and shaped, and obturation was completed using ProTaper Gold gutta-percha with AH Plus sealer (Dentsply, Konstanz, Germany) (Fig. 8).
Periapical radiograph of tooth 36 with obturation on DB and DL canal. Sealer extrusion noted.
Hemisection and removal of the mesial root were performed under local anesthesia. Hemisection was chosen because the lesion involved only one root, while the remaining distal root had sufficient alveolar bone support. The tooth also had strategic value as a terminal abutment, critical for maintaining stable occlusion. A full-thickness flap was elevated on the buccal and lingual aspects. Using a low-speed surgical fissure carbide bur under normal saline irrigation, a vertical cut was made to separate the tooth. The mesial root was elevated and removed, and granulation tissue in the mesial socket was curetted. The socket was irrigated with sterile saline, and the flap was approximated and sutured with Vicryl 4–0 sutures (Fig. 9). The occlusal table was minimized to direct forces along the long axis of the distal root. Immediate postoperative radiographs confirmed the stable retention of the distal root (Fig. 10).
Clinical photographs showing (a) line of resection through furcation area and separation of mesial and distal segments, (b) surgical field after removal of resected half of tooth structure, (c) surgical field after suturing, (d) 2 weeks postoperative showing healing of soft tissue.
Immediate postoperative radiograph of the mesial segment of tooth 36 showing overhanging dentin at furcation area mesial to the remaining root.
Follow-up at three months showed no symptoms, tenderness to percussion, swelling, periodontal pocketing, or mobility. This aligns with evidence suggesting that periodontal tissue maturation occurs within three months post-surgery [8]. Subsequently, tooth 35 and the distal segment of tooth 36 were prepared for a milled PFM bridge in preparation for upper and lower cobalt-chrome partial dentures. The design included a premolar pontic, a mesial rest seat on tooth 35, and a lingual rest seat on both teeth 35 and 36 (Fig. 11 and 12).

Clinical photographs showing the occlusal view of milled PBM bridge 35-P-36 after cementation.
Periapical radiograph post-cementation of bridge 35–36 showing good adaptation of restorative margins and healing of bony lesion.
Discussion
The prognosis of hemisection procedures has been well-documented in the literature, but the reported data vary greatly. While some studies report survival rates exceeding 90%, others report rates ranging between 40% and 60%. These significant variations can be attributed to differences in inclusion criteria, outcome definitions, follow-up periods, maintenance protocols, and restorative methods. In a recent systematic review by Mokbel et al. [9], it was noted that despite the variability in reported outcomes, more than half of the retrospective studies reported survival rates greater than 90%, with follow-up periods extending up to 23 years.
Hemisection is a technique-sensitive procedure, requiring meticulous attention throughout the processes of case selection, root canal treatment, surgery, and restorative and maintenance therapies. Atraumatic separation, favorable anatomy, conservative root canal therapy, patient maintenance of good oral hygiene, and adequate periodontal support around the residual root are critical for success. The absence of specific inclusion criteria for optimal case selection may have led some authors to retain questionable teeth, resulting in reduced survival rates. Lee et al. (2012) used resective therapy as a last-resort intervention and was not selective in case inclusion. Various factors, such as reduced pre-operative radiographic bone heights around the surviving root, grade II or higher mobility, and advanced patient age, negatively influence the survival of molar teeth after resection [10].
The decision to use a hemisected tooth as an abutment for a fixed partial prosthesis remains a topic of debate. The reduced periodontal support following root removal exposes the remaining root to deflection during function, particularly when a single cantilevered prosthesis is constructed. To enhance the longevity of the hemisected tooth, splinting it to an adjacent tooth for redistributing occlusal forces is recommended [11]. Research indicates that the prognosis of hemisected teeth can be comparable to conventionally root canal-treated teeth [12].
In recent decades, dental implants have gained popularity, with 5-year survival rates for single-crown implants and implant-supported fixed dental prostheses (FDPs) estimated between 97.7% and 93.6% and 10-year survival rates between 94.9% and 86.7% [13]. However, compromised teeth that might previously have been preserved are often extracted and replaced with implants. This trend raises concerns, as implants, while promising, are invasive, financially demanding, and not free from complications. A systematic review by Derks et al. (2015) reported
a prevalence of peri-implant mucositis and peri-implantitis at 65% and 47%, respectively, with treatment of these complications proving challenging and unpredictable [14].
Direct comparisons between hemisection and implant treatment approaches are challenging. In a retrospective comparison, Fugazzotto reported cumulative success rates of 96.8% for root-resected molars and 97% for molar implants, indicating high functional success for both methods [11]. Maintaining an inflammation-free environment in a molar reduces additional bone loss, which might compromise future implant placement. This supports the use of conservative resective procedures, particularly in younger patients, delaying implant placement until later in life. Hemisection and root resection provide advantages, including preservation of alveolar morphology and psychological benefits of over-extraction, as part of the tooth is retained. From a financial perspective, resective procedures are often less expensive than implants [15]. Furthermore, proximity to anatomical landmarks such as the maxillary sinus or inferior alveolar canal can limit the feasibility of implants, necessitating additional surgeries. In such cases, resective procedures offer a safe and effective alternative [9].
Park et al. [16] evaluated factors influencing outcomes of root-resective procedures in a 10-year retrospective study, emphasizing the importance of prosthetic design in preventing fractures and biomechanical failures. Molar roots, being narrower mesiodistally and wider buccolingually, require specific modifications in preparation design. A flat emergence profile from the preparation margin, under-contouring of embrasure spaces, and an occlusal scheme with a narrower table and reduced cuspal inclines are essential for minimizing occlusal loads [9]. Splinting resected teeth to adjacent teeth significantly reduces the incidence of tooth loss by 74% compared to unsplinted restorations [10].
Given the ongoing debate surrounding the use of hemisected teeth as abutments, dental professionals must evaluate each case individually and consider alternative treatments aligned with the patient’s circumstances and long-term goals. Both presented cases were restored with fixed splinted dental prostheses. In case one, the resected root was restored as a molar, while in case two, it was restored as two premolars. Despite differences in design, the restorations adhered to the basic principles of minimizing occlusal loads on the resected root.
Conclusion
Root resection and hemisection are reliable and predictable treatment modalities that should be considered viable alternatives to tooth extraction in appropriate cases. With meticulous case selection, careful root canal treatment, well-planned restorative design, and adherence to a robust maintenance program, molars involved in such procedures can achieve prolonged survival with high success rates. These conservative approaches not only preserve natural dentition but also offer significant functional, psychological, and financial benefits.
Conflict of interest statement
The authors declare no conflict of interest.
Funding
No external funding was received.
Informed consent
Written informed consent was obtained for all participants.
Consent for publication
Written informed consent was obtained from patients to publish these cases.
Data availability
The data supporting this study’s findings are available from the corresponding author upon reasonable request.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}