





Abstract
Ventral hernias are common abdominal wall defects; however, the presence of complicated diverticulitis within a hernia sac is exceedingly rare. We report the case of a 76-year-old female with multiple comorbidities who presented with acute left-sided abdominal pain and a tender, irreducible mass. Computed tomography imaging revealed a left lateral ventral hernia containing an inflamed diverticulum of the transverse colon. The patient underwent emergency hybrid laparoscopic surgery involving hernia sac resection, diverticulectomy, and primary abdominal wall repair. Her postoperative course was uneventful, and she was discharged on Day 5. This unusual presentation mimics both incarcerated hernia and acute diverticulitis, complicating diagnosis. Early imaging and prompt surgical management are vital to prevent life-threatening complications such as strangulation or perforation. This case emphasizes the importance of clinical awareness and individualized surgical strategies in managing complex ventral hernias. A multidisciplinary approach is essential for optimizing outcomes in rare and challenging abdominal emergencies.
Introduction
Ventral hernias (including both primary and incisional) are estimated to affect ~10%–15% of adults at some point in their lives, with incisional hernias alone occurring in up to 20% of patients following abdominal surgery [1]. Ventral hernias not only pose a risk of incarceration and strangulation but also account for a substantial healthcare burden, with over 350 000 ventral hernia repairs performed annually in the United States alone [2]. Hernias are classified into several types based on their location. Ventral hernias occur in the anterior (front) abdominal wall and form when the muscles in the abdominal wall weaken or when an opening develops, allowing tissue or intestines to protrude through [3].
The presence of complicated acute diverticulitis within a ventral hernia is extremely rare [4]. The clinical significance of such a presentation lies in the increased risk of incarceration and strangulation, which can lead to life-threatening complications if not promptly treated [5]. To the best of our knowledge, this case report presents the first known instance of a strangulated ventral hernia sac containing an inflamed diverticulum of the transverse colon, highlighting the importance of heightened clinical suspicion and early surgical management.
Case presentation
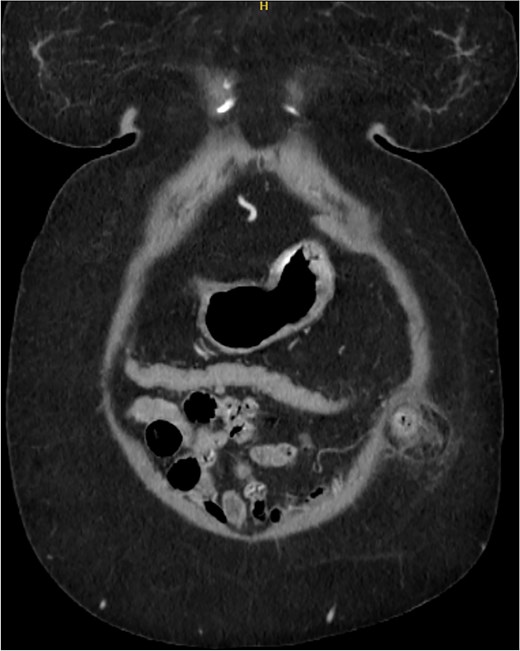
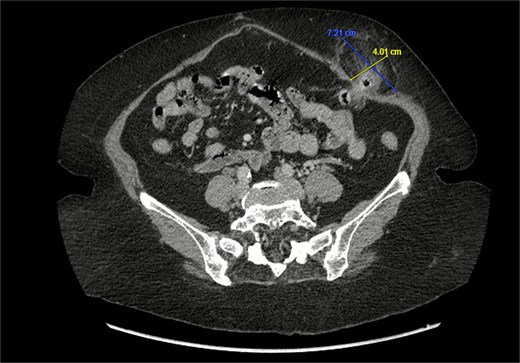
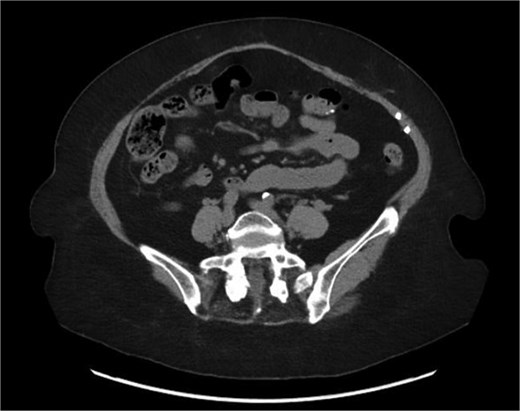
A 76-year-old female with a medical history of type 2 diabetes mellitus (controlled with oral medications), hypertension (on two medications), hyperlipidemia (on atorvastatin), and recently diagnosed Alzheimer’s disease (started on memantine) presented to the emergency department with severe left-sided abdominal pain of 2 days’ duration. The pain began gradually but worsened significantly in the last few hours. It was associated with a bulging mass in the abdomen that was tender and painful to touch. The patient reported that the swelling had been present for 2 years, intermittently reducible with minimal exertion. However, since the previous day, it had become irreducible and increasingly painful, particularly after a failed attempt to reduce it manually at home. She also admitted to chronic constipation for years, usually treated with oral laxatives, though she had not been compliant with them recently. Her surgical history included a laparoscopic cholecystectomy combined with paraumbilical hernia repair using mesh 3 years ago. Upon examination by the on-call surgical team, the patient was afebrile with stable vital signs. Her abdomen was distended, and a 7 × 7 cm irreducible, tender mass was noted over the left side. An urgent computed tomography (CT) scan of the abdomen and pelvis with intravenous and oral contrast revealed a left lateral ventral abdominal hernia traversing the left lateral oblique muscles. The hernia sac contained omental fat and an inflamed diverticulum of the transverse colon, with surrounding inflammatory changes. The defect measured 1.4 × 1 cm, and the hernia sac measured 6.7 × 4.2 × 4 cm. No free fluid, fluid collections, or pneumoperitoneum were identified (Figs 1–3).
Axial section of the CT showing the ventral hernia diameter.

Coronal section of CT abdomen and pelvis showing the ventral hernia.
Sagittal section of CT abdomen and pelvis showing the ventral hernia.
The patient was immediately taken to the operating room for emergency surgery. Preoperatively, prophylactic anticoagulation (heparin 5000 IU subcutaneously) and antibiotics (2 g of first-generation cephalosporin) were administered. Under general anesthesia, the patient was positioned supine, prepped, and draped using standard sterile technique. Laparoscopic entry was achieved via optical technique using a 5-mm Vesiport. Three additional ports were inserted under direct visualization. Intraoperatively, the old mesh was noted over the umbilicus, with omental adhesions. A ventral hernia was found between the muscle layers, containing omental fat and an inflamed diverticulum from the transverse colon. Extensive adhesolysis and hemostasis were performed using the LigaSure device. The diverticulum was resected and closed with an ENDO-GIA purple stapler. A 7-cm transverse incision was made over the left lateral abdominal wall as part of a laparoscopic hybrid approach to allow hernia sac resection and closure of the defect in layers. The abdomen was deflated, skin sutured, and the patient was successfully extubated.
Postoperatively, the patient had an uneventful course and was discharged on Day 5. At the 6-month follow-up, she remained asymptomatic. A CT scan performed at her request for reassurance showed no signs of recurrence or acute abdominal pathology (Figs 4 and 5).
Axial section of the CT 6 months after the surgery.
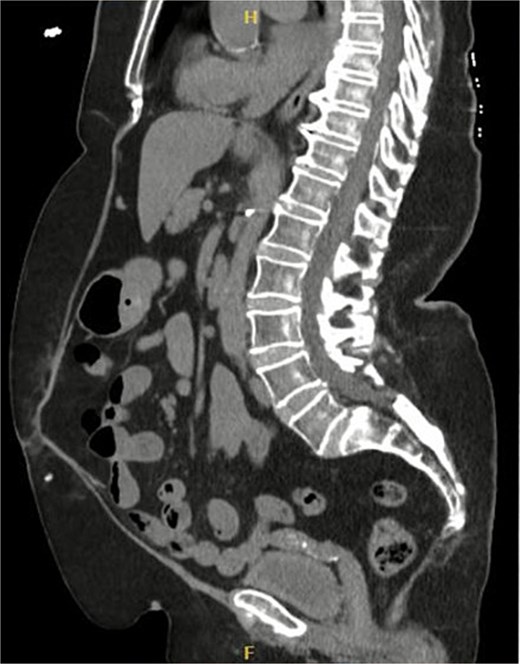
Sagittal section of CT abdomen and pelvis 6 months after the surgery.
Discussion
This case highlights the intersection of two distinct but common conditions: ventral hernia and diverticulitis. Ventral hernias occur through defects in the anterior abdominal wall and may be caused by chronic diseases like diabetes, chronic constipation, obesity, chronic coughing (e.g. in asthmatics or smokers), heavy lifting, multiple pregnancies, abdominal trauma, or previous surgeries [3, 6]. Symptoms can range from asymptomatic masses to painful, irreducible bulges associated with nausea, vomiting, or obstruction.
While ventral hernias themselves are not rare, the contents of the hernia sac can be unusual. In our literature review, we found only a handful of cases describing diverticulitis within hernia sacs (Table 1). One case involved a Bochdalek hernia with an incarcerated splenic flexure [3, 7], and two cases involved Spigelian hernias mimicking diverticulitis [8, 9]. Of 10 documented cases where diverticulitis was the content of groin hernias [10], one involved the cecum, one the transverse colon, and the rest the sigmoid colon [3, 7, 11]. No cases of ventral hernias containing an inflamed transverse colon diverticulum were found—making this report, to our knowledge, the first of its kind.
Hernia types and its content
| Hernia type | Content identified | Number of cases | Notes | References |
|---|---|---|---|---|
| Bochdalek hernia | Incarcerated splenic flexure of the colon | 1 | Rare case found in literature | [3, 7] |
| Spigelian hernia | Mimicking diverticulitis | 2 | Initially misdiagnosed as diverticulitis | [8] |
| Groin hernia | Diverticulitis (any location) | 10 | Increasingly documented in recent years | [3, 7] |
| Cecal diverticulitis | 1 | Subtype of groin hernia case | [3, 7] | |
| Transverse colon | 1 | Another groin hernia subtype | [3, 7] | |
| Sigmoid colon | 8 | Majority of documented groin hernia diverticulitis cases | [3, 7] | |
| Ventral hernia | Inflamed diverticulum of transverse colon | 0 (previously) | No prior cases documented before our report | — |
Diverticula form at weak points in the colonic wall where blood vessels penetrate the muscle. Most are ``false'' diverticula, consisting of mucosa and submucosa herniating through the muscle layer, covered only by serosa. In contrast, true diverticula (e.g. Meckel’s) contain all layers of the bowel wall [12]. Diverticulitis occurs when diverticula become inflamed or perforated, often due to obstruction or increased intraluminal pressure. While sigmoid colon involvement is most common, diverticulitis of the transverse colon is particularly rare—occurring in less than 6% of Western populations [13].
Clinically, this combination of strangulated hernia and diverticulitis can produce overlapping symptoms: localized abdominal pain, irreducible hernia mass, nausea, vomiting, and sometimes systemic signs like leukocytosis or fever. This makes diagnosis challenging [14]. Cross-sectional imaging, particularly CT, plays a crucial role in distinguishing between simple hernias and more complex presentations like the one reported here.
Laparoscopic or hybrid approaches allow excellent visualization, safe resection of inflamed tissue, and layered closure of hernia defects. Early surgical intervention is essential to avoid severe complications such as perforation, sepsis, or peritonitis.
Conclusion
This case highlights an extremely rare presentation of a strangulated ventral hernia containing an inflamed diverticulum of the transverse colon. While both conditions are common separately, their coexistence in this manner is exceptional. Early diagnosis via imaging and prompt surgical management are critical to prevent serious complications.
Clinicians should maintain a high index of suspicion in elderly patients with longstanding hernias and new-onset abdominal pain. Timely recognition and appropriate surgical intervention can lead to favorable outcomes, even in rare and complex presentations like this one.
Conflict of interest statement
None declared.
Funding
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}