





Abstract
Endometriosis of the vermiform appendix is an uncommon pathology that may present as an appendiceal mass identified on colonoscopy. This may be due to an appendiceal endometrioma or intussusception of the appendix. Mucinous appendiceal neoplasms and neuroendocrine tumors are important clinical differentials. When there is concern for possible malignancy, resection is recommended, usually as a stapled cecectomy. In this case we describe an appendiceal endometrioma presenting as an appendiceal mass, requiring a right hemicolectomy.
Introduction
The appendix is an uncommon location for endometriosis, usually at the tip of appendix identified during diagnostic laparoscopy. Endometriosis of the appendix may present clinically as appendicitis [1] or be found incidentally during surgery for endometriosis, occurring in 7.23% of cases. An Australian study identified endometriosis in 0.61% of 2284 female appendicectomy specimens, of which 39.5% had concurrent appendicitis, and 14.3% had a concurrent mucinous neoplasm [2].
A rare presentation of appendiceal endometriosis is as a mass at the appendiceal orifice. Differentials for an appendiceal mass include fecaliths, parasites, foreign bodies, polyps, malignancy, and, in our case, endometriosis [3]. Endometriosis of the appendix may develop a mass-forming endometrioma [4] or act as a lead point for intussusception of the appendix [5]. Endometriosis is the most common (33%) cause of appendiceal intussusception in adults [6], and has been described to present clinically as a mimic for appendicitis [3], or as a mass at the appendiceal orifice identified during endoscopy [5, 7]. In both cases, imaging is often inconclusive, and intra-operatively, the appendix may not be identifiable at the convergence of the taenia coli.
In this case, we describe a case of an appendiceal endometrioma mimicking an appendiceal neoplasm as a mass at the appendiceal orifice.
Case report
A 40-year-old female was referred to a colorectal surgeon for workup of altered bowel habits in the setting of endometriosis. She described increasing constipation and hard stools over several months. She denied per-rectal bleeding or loss of weight. There were no abnormalities on abdominal or rectal examination. She had previously undergone diagnostic laparoscopy for endometriosis, which had revealed pelvic adhesions. No tethering of the right colon or appendix was noted at the time. The patient was being considered for hysterectomy to treat chronic pelvic pain and dysmenorrhea secondary to endometriosis. She was taking hormone replacement therapy for endometrial suppression.
As part of pre-operative workup, a colonoscopy was performed, revealing an abnormal appendiceal orifice with an intraluminal protruding “fish mouth” mass suspicious for an appendiceal mucinous neoplasm (Fig. 1). Of note, there was no mucin identified. A cold snare biopsy was taken of a polyp overlying the mass, with histological examination demonstrating a sessile serrated lesion. Subsequent CT and MRI of the abdomen did not definitively identify the appendix. No caecal abnormality for free fluid was demonstrated.
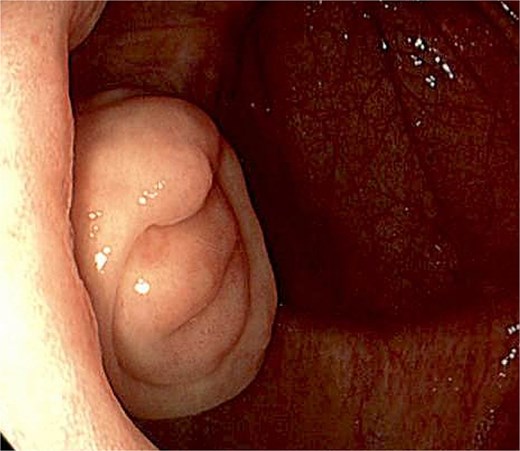
Colonoscopic image of protruding, intraluminal, “fish mouth” appearing mass at the appendiceal orifice.
To obtain a tissue diagnosis and exclude an appendiceal mucinous neoplasm, the patient was planned for laparoscopic cecectomy. Intraoperative findings included pelvic adhesions (Fig. 2), a short appendix and a firm caecal base suspicious for malignancy (Fig. 3). A partial cecectomy was unable to be performed with appropriate margins, and right hemicolectomy was performed instead with side-to-side stapled ileocolic anastomosis. The patient’s recovery was uncomplicated, and she was discharged day 4 postoperatively.
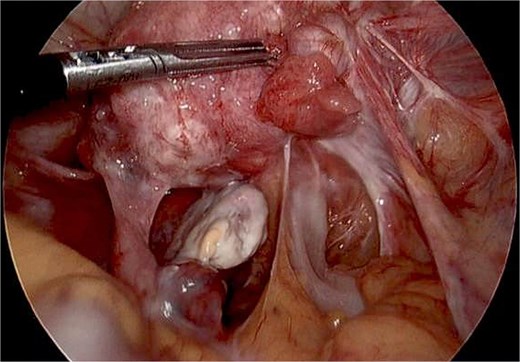
Intraoperative image of pelvic adhesions secondary to endometriosis. No mucin was seen.
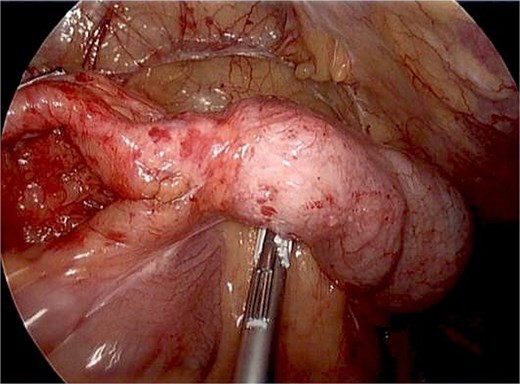
Intraoperative image of thickened caecum without any obvious mass on the serosal surface of colon and shortened appendix.
Macroscopic examination of the resected caecum showed a small appendiceal stump with an intraluminal nodule at the appendiceal orifice (Fig. 4). Transection of the appendiceal remnant showed a firm, white structure. Microscopic examination revealed multiple foci of endometriosis within the muscularis mucosae, muscularis propria (Fig. 5), submucosa, and mesentery of the appendix. There was no neoplasia identified in the appendix or 33 lymph nodes.

Transected ileocolic resection specimen with intraluminal view, arrow indicating appendiceal nodule.
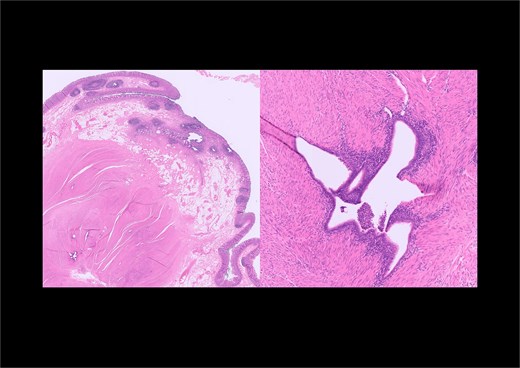
Low and high-power microscopic views of the appendix showing foci of endometriosis within the muscularis propria.
Discussion
Fish mouth appearance of appendiceal orifice is highly suggestive of mucinous appendiceal neoplasm. However, when mucin is absent, other differentials should be considered.
Differentials for an appendiceal mass include endometriosis, malignancy, and appendiceal intussusception. Endometriosis may exist concurrently with an appendiceal neoplasm [8], or an appendix that macroscopically appears consistent with endometriosis may represent malignancy [9]. Therefore, surgical resection is the recommended treatment for an appendiceal mass.
In the case of appendiceal intussusception, the appendix may be absent at the convergence of the taenia coli and instead present as a mass at the caecal base. Reduction of the appendiceal intussusception to facilitate appendicectomy has been described, but more commonly, stapled cecectomy is required. As described in this case, if there is concern for malignancy and a stapled cecectomy cannot be performed with appropriate margins, a right hemicolectomy may be required [5].
Appendiceal intussusception is an uncommon pathology that may present as an appendiceal mass found on colonoscopy. It is most frequently caused by endometriosis in adult females; however, surgical resection may be required to exclude neoplastic differentials such as appendiceal mucinous neoplasms and neuroendocrine tumors.
Conflict of interest statement
None declared.
Funding
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}