





Abstract
Squamous cell carcinoma is the most common primary malignancy of palatine tonsils, and usually it is associated with smoking, alcohol consumption, and human papilloma virus infection. Metastatic tonsillar carcinoma is extremely rare with range between 0.8% and 1% of all tonsillar carcinoma, and most cases emerge from the skin, kidney, lung, stomach, and breast. To the best of our knowledge, metastatic involvement of the palatine tonsil originating from urinary bladder carcinoma has not been previously reported in the literature. We present a 72-year-old male with locally advanced urinary bladder cancer, subsequently diagnosed with metastatic palatine carcinoma. Histopathology confirmed urothelial carcinoma sparing lymph nodes. The patient died due to cardiac condition after 8 months of his diagnosis. Metastatic tonsillar cancers are extremely rare, especially from unexpected tumors such as urinary bladder cancer.
Introduction
Squamous cell carcinoma is the most common primary malignancy of palatine tonsils, and usually it is associated with smoking, alcohol consumption, and human papilloma virus infection [1]. On the other hand, metastatic tonsillar carcinoma is extremely rare with range between 0.8% and 1% of all tonsillar carcinoma [2–4]. Additionally, most of the cases emerge from the skin, kidney, lung, stomach, and breast [2]. To the best of our knowledge, metastatic involvement of the palatine tonsil originating from urinary bladder carcinoma has not been previously reported in the literature. In our case, we present a 72-year-old male with a history of locally advanced urinary bladder cancer, who was subsequently diagnosed with metastatic palatine carcinoma. Histopathological examination confirmed urothelial cell carcinoma, notably with sparing of the regional lymph nodes.
Case presentation
A 72-year-old male, presented to Head and Neck surgery clinic in a tertiary hospital, Dammam, Saudi Arabia. Patient referred to us as a case of multiple parotid lesions with fine needle aspiration result of Warthin tumor. Additionally, he has a left tonsillar mass. Upon examination, the patient has asymmetrical palatine tonsils with ulceration over the left tonsillar fossa. Regarding past surgical and medical history, patient is known to have uncontrolled hypertension and diabetes mellitus type 2, ischemic heart disease status post coronary artery bypass graft surgery 8 years prior to the presentation, chronic obstructive pulmonary disease associated with obstructive sleep apnea, locally advanced bladder cancer T3N3M1 according to TNM staging system for bladder cancer, status post neoadjuvant chemotherapy followed by surgical transurethral resection of bladder tumor and radical concurrent chemoradiotherapy.
Additionally, the patient had done computed tomography (CT) scan for chest, abdomen, and pelvis, and CT neck with contrast.
CT scan neck with contrast (Figs 1 and 2):
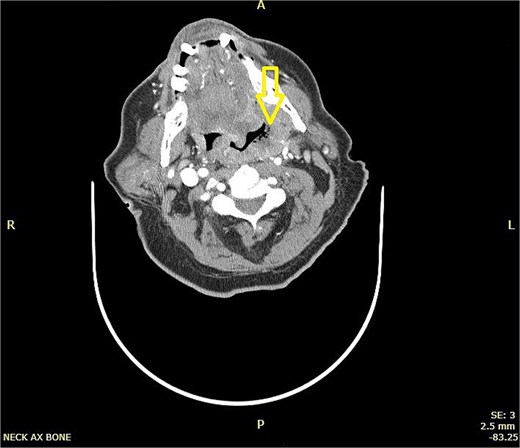
CT scan of neck showing a hyper-dense lesion in the tail of the right parotid gland measuring 1.3 × 0.9 cm (AP, TV dimensions) with no deep extension. The left tonsil is enlarged with faint, il-defined rim enhancement, and central air foci, indicating early abscess formation.

CT scan of neck showing a hyper-dense lesion in the tail of the right parotid gland measuring 1.3 × 0.9 cm (AP, TV dimensions) with no deep extension. The left tonsil is enlarged with faint, il-defined rim enhancement, and central air foci, indicating early abscess formation.
Impression:
CT left parotid hyper-dense lesion, which may indicate lymph node metastasis or primary tumor. For pathological correlation (which showed Warthin tumor) and early left tonsillar abscess for clinical correlation.
CT scan Chest, abdomen, and pelvis with contrast:
Impression:
Compared with an old CT scan showing slight interval progression of mild circumferential diffuse urinary bladder mural thickening without suspicious focal lesion, interval stability of the iliac lymph nodes, and Interval regression in size of the previously seen hypo-dense splenic lesion.
Furthermore, the patient went for left side tonsillectomy for biopsy. Histopathology report showed squamous mucosa ulcerated by poorly differentiated carcinoma with heavy intratumoral neutrophilic infiltration, a histomorphology that is identical to the patient known urinary bladder primary carcinoma.
To add on, the patient was admitted to intensive care unit after 7 months of first presentation to our clinic with history of falling, diagnosed with pulmonary edema, and decompensated heart failure. Moreover, palliative care offered, and do not resuscitate form signed. Unfortunately, patient arrested and died due to his cardiac condition after 8 months of his diagnosis with tonsillar metastatic carcinoma.
Discussion
Bladder cancer is a significant contributor to morbidity and mortality, it is considered the sixth most common malignancy in the United States [5]. Urothelial carcinoma is the predominant subtype accounting for ~95% of the cases and tends to be less aggressive than non-urothelial bladder carcinomas [6]. Moreover, bladder cancer commonly metastasizes to lymph nodes followed by bone and lungs [7]. Therefore, tonsillar metastasis is not a usual location for urinary bladder cancer. Regarding primary tonsillar carcinoma, it is a common malignancy within head and neck region and accounts for 15%–20% of oro-pharyngeal cancers [8]. On the other hand, secondary tumor metastasis to tonsils is extremely rare, according to multiple studies only 0.8%–1% had been reported [2–4]. In our case, urothelial carcinoma had not been reported previously in the literature as a metastasis to the palatine tonsil. Oligometastasis is defined as state of cancer patients have 1–5 metastatic lesions with active primary disease [9]. Our case is deemed oligometastatic with only one lesion presented in the left palatine tonsil sparing lymph nodes and body tissues all the way. Mechanisms regarding metastasis of non-head and neck tumors to the palatine tonsils are not fully understood. But there are multiple hypotheses explaining the way of spread: the first one is retrograde transportation of the tumor cells due to lack of efferent lymphatic drainage in the palatine tonsils, and this is the only possible in the absence of cervical lymphatic metastasis [3]. The second hypothesis is hematogenous spread, which is suggested to be characteristic of primary abdominal tumors. In this pathway, tumor cells bypass hepatic and pulmonary filtration via the portal circulation, subsequently reaching the heart and disseminating to the tonsils through the systemic circulation [10]. While third hypothesis showing that tumor cells can reach head and neck region by passing the lungs via paravertebral venous plexus (Baston’s plexus) [11]. Metastasis to palatine tonsils typically unilateral with preference of the left side as our case presentation and there is no explanation or theory for this finding [12]. Furthermore, patients with tonsillar metastatic mass may vary with their symptoms, such as dyspnea, pain, bleeding, or discomfort and even they could be asymptomatic with sudden examination finding which usually causes delay in diagnosis and management. Tonsillar metastasis is considered a systemic malignant tumor metastatic disease and should be treated accordingly to achieve possible long term survival [3, 13]. Moreover, metastatic tonsillar cancers commonly carry a poor prognosis regardless of the primary tumor and the treatment provided [10]. The overall average survival time reported by Huang et al. literature review is ranged between 4 and 12 months, and it is compatible with our patient survival time which equals 8 months [2].
Conclusion
Metastatic tonsillar cancers are extremely rare, especially from non-expected tumors such as urinary bladder cancer. Additionally, absence of lymphadenopathy in diagnosed cancer patients with a presentation of unilateral tonsillar mass or ulcer must be investigated to rule out metastatic diseases.
Conflict of interest statement
None declared.
Funding
None declared.
Ethical approval
This study did not require ethical approval as it is a case report.
References
Mastronikolis NS, Tsiropoulos GE, Chorianopoulos D, et al. Palatine tonsillar metastasis from lung adenocarcinoma. Eur Rev Med Pharmacol Sci 2007;11:279–82.

{kind=link}
{kind=link}