





Abstract
Renal artery pseudoaneurysm (RAP) formation following flexible ureterorenoscopy (FURS) with laser lithotripsy is rare. Previous kidney surgery places patients at an increased risk due to potential vascular injury associated with renal intervention. In our case, a 62-year-old man with a single functioning right kidney and a history of right partial nephrectomy presented 10 days following FURS with holmium laser lithotripsy, complaining of gross hematuria. Attempted conservative management failed. Renal arteriography was done, which revealed a RAP that was managed with selective angioembolization. RAP following FURS can be serious if not managed properly. Most cases present with late gross hematuria. RAP can usually be demonstrated on renal arteriography. Selective angioembolization is the definitive treatment.
Introduction
Flexible ureterorenoscopy (FURS) with laser lithotripsy is considered the first choice for the management of kidney stones ≤2 cm [1]. It is a minimally invasive treatment modality with a relatively low complication rate [2]. Renal artery pseudoaneurysm (RAP) has been rarely reported after uncomplicated FURS with laser lithotripsy [3]. We herein report a case of RAP developed after uncomplicated FURS and Holmium laser lithotripsy in a single functioning kidney. It was managed with selective angioembolization.
Case report
A 62-year-old man presented to the urology clinic complaining of recurrent right flank pain and an ultrasound report of a right kidney stone. Patient had a history of left open pyelolithotomy performed twice due to left kidney stone, which led to left atrophic kidney. He had a history of right open partial nephrectomy due to renal mass highly suspicious of renal cell carcinoma on CT done 4 years ago. He had a medical history of type 2 diabetes mellitus, hypertension, dyslipidemia, and stage I chronic kidney disease (CKD). A new noncontrast CT showed left atrophic kidney and right huge kidney stone of 4.5 × 4 cm in the posterior part of the upper calyx (Fig. 1). Patient was offered percutaneous nephrolithotomy (PCNL), but he refused due to the fear of possible bleeding complications. He preferred multiple session flexible ureteroscopy with holmium laser lithotripsy. The patient was pre-stented 2 weeks before the first session.
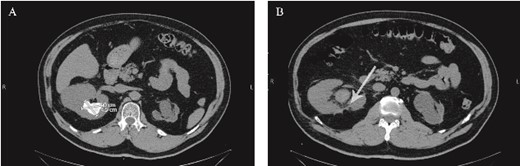
(A) Preoperative non-contrast CT scan showing a renal stone measuring 4.5*4 cm. (B) Postoperative non-contrast CT scan. The arrow points to the area from which the pseudoaneurysm most-likely originated postoperatively.
The ureteral access sheath was placed under fluoroscopy guidance. After that, a disposable flexible ureteroscope was introduced. The stone was identified and disintegrated with a low-energy holmium laser machine (30 W) in dusting mode. Total procedure time was 60 min. A double J stent was inserted, and the first session ended uneventfully.
Ten days after discharge, the patient presented to the emergency department (ED) due to gross hematuria. Patient was hemodynamically stable with a hemoglobin drop from 12 on discharge to 10.7 at the ED. Foley’s catheter was applied, and continuous irrigation was performed, which showed persistent gross hematuria. Contrast-enhanced CT was able to identify a faint contrast extravasation at the posterior surface of the kidney, which was reported to be suspicious of vascular complications. Conservative management with blood product transfusion and antifibrinolytic agents was decided. Hematuria subsided 3 days later, and the patient was discharged the following day with a hemoglobin of 11.9.
Eight days after discharge, he presented to the ED complaining of gross massive hematuria. He went into cardiac arrest, and cardiopulmonary resuscitation (CPR) was performed. His hemoglobin had dropped from 11.9 on the day of previous discharge to 6.8. He was later stabilized and started on blood transfusion and was put under close observation until he became hemodynamically stable. He underwent emergent renal arteriography, which showed RAP, and selective angioembolization was done (Fig. 2). Hematuria subsided after 2 days, and the patient was discharged. After 3 months, the patient was well and still in stage I CKD.
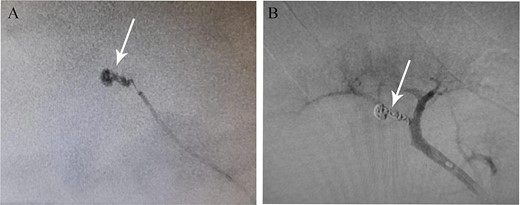
(A) Pseudoaneurysm seen on renal angiography. (B) The pseudoaneurysm following angioembolization.
Discussion
The miniaturization of equipment accompanied with the development and advancement in laser technology has facilitated the usage of FURS in the treatment of variable sizes of kidney stones [7]. With its lower vascular complication rate compared to percutaneous nephrolithotomy, it is gaining more popularity despite being an expensive treatment modality [8].
One of the rare vascular complications is RAP, which occurs after focal rupture of the renal artery wall or its branches. This will lead to the formation of a localized hematoma surrounded by a thin fibrin wall, which upon rupturing, will result in massive bleeding [3]. There are few case reports regarding RAP after FURS with laser lithotripsy (Table 1) [3–6]. Commonly, it presents with late massive hematuria, which can be life-threatening if left untreated [9]. In our case, the patient presented with gross hematuria after 10 days of his FURS procedure. Contrast-enhanced CT is beneficial in the diagnosis, but definitive conclusions and interventions are best made using renal arteriography. In our patient, contrast-enhanced CT showed contrast extravasation with high suspicion of RAP. Renal arteriography confirmed the diagnosis of the pseudoaneurysm.
Cases reported in the literature of RAP following flexible ureteroscopy and holmium laser lithotripsy.
| Case | Sex | Age | Type of intervention | Comorbidities | History of prior renal surgery | Onset of complications |
|---|---|---|---|---|---|---|
| Durner et al. (2015) [4] | M | 56 | FURS + holmiumYAG laser | Mitral heart valve replacement | None | N/A |
| Bashar & Hammad (2019) [5] | M | 79 | FURS + holmium laser | DM + HTN + stage 4 CKD + valvular heart disease | Previous ESWL and FURS with Holmium laser lithotripsy | 4 days later |
| Deng et al. (2022) [3] | M | 29 | FURS + holmium laser | Diabetes for 2 years | None | 28 days later |
| Yin et al. (2023) [6] | M | 53 | FURS + holmium laser | None | Open bilateral nephrolithotomy (33 years ago) + bilateral inguinal hernia repair (1 month ago) | 8 days later |
CKD, chronic kidney disease; DM, diabetes mellitus; ESWL, Extracorporeal shock wave lithotripsy; FURS, flexible ureterorenoscopy; HTN, hypertension; NSTEMI, nonST elevation myocardial infarction; N/A, not available.
The formation of RAP after FURS is caused by multiple factors and not attributed to a single cause. The factors include direct renal damage, increased intrarenal pressure, prolonged operation time, high laser energy, and lastly, previous kidney surgery [9]. The type of the laser, whether holmium or thulium laser, probably does not affect the possibility of RAP formation, as there are case reports related to RAP formation after FURS with thulium laser technology [9]. Our patient had a history of open partial nephrectomy due to kidney mass in the posterior surface. Renal arteriography demonstrated the RAP to be in the posterior branches of the renal artery, which is highly suggestive that previous surgery led to alteration in the intrarenal anatomical course of the vasculature and thinner renal parenchyma in the operation site, which increased the risk of intrarenal vascular damage even with an unintentional mucosal low-energy laser insult. Therefore, urologists could be very careful when deciding and doing FURS with laser lithotripsy in patients with previous kidney surgery.
Selective angioembolization is considered a definitive treatment modality because it is minimally invasive with little harm to kidney function [10]. Open repair is the choice when angioembolization fails or if the patient is hemodynamically unstable. Conservative management of RAPs with blood products, transfusions, and antifibrinolytic agents was reported in a few cases with trauma-related RAPs and was enough to control the situation [11]. Despite the possibility of conservative management of RAPs, intervention could be more appropriate because it is hard to predict the outcome. As in our case, conservative management failed and could lead to fatal consequences.
Renal pseudoaneurysm is a rare and unusual complication after FURS with laser lithotripsy. It presents with late gross massive hematuria, which could be life-threatening if not recognized or suspected. Good selection of cases, minimizing operation time, maintaining a normal intrarenal pressure, avoiding direct laser contact with mucosa, and using low energy are the main preventing modalities.
Conflict of interest statement
None declared.
Funding
No external funding was provided.

{kind=link}
{kind=link}