





Abstract
Reconstructing ear defects in very elderly patients is challenging, but one-step procedures are beneficial due to reduced morbidity and fewer hospital visits while maintaining ear size, shape, and symmetry. In 2018, Jaber et al. introduced a 90° earlobe rotation technique to repair full-thickness auricular defects while preserving the earlobe. We present a modified approach, dividing the earlobe into two flaps for better mobility, rotating them to cover a mid-helix defect in a 93-year-old patient. This is especially useful for older patients with large earlobes, who are prone to skin cancers like keratinocyte cancer. The cosmetic result is satisfactory, with minor asymmetries rarely an issue. This technique provides a practical, single-step solution for functional and esthetic reconstruction in elderly patients.
Introduction
While the primary objective of ear reconstruction is to maintain the ear's size, shape, and symmetry, reconstruction in elderly patients presents challenges, as a one-step repair is often necessary due to limited mobility and difficulties with patient transportation. Fortunately, minor asymmetries between the ears generally go unnoticed, as both ears are rarely observed simultaneously [1].
In 2018, Jaber et al. introduced a surgical technique for reconstructing full-thickness defects in the middle portion of the auricle, including the helix and antihelix, extending to the adjacent concha, while preserving the entire earlobe. This single-stage procedure involves rotating the earlobe 90° to reconstruct these defects, suturing it in place, and potentially performing a triangular wedge excision if there is a discrepancy between the defect and the available tissue. This technique is particularly suitable for elderly patients with large, pendulous earlobes. Moreover, this demographic has the highest incidence of skin cancer, especially keratinocyte cancer [2].
The earlobe consists of two thick layers of skin separated by adipose and dense connective tissue. Although it lacks cartilage, its dense subcutaneous tissue can bring structure to the helix in auricle reconstruction. The earlobe is supplied with blood by the inferior and medial branches of the superficial temporal artery and a branch of the posterior auricular artery, classifying it as an axial skin flap. There are two primary anatomical types of earlobes: pendulous (free from the cheek) and attached. This technique is ideal for the pendulous type [2].
Case presentation
We present the case of a 93-year-old patient with a 1.2 cm full-thickness ear defect following a wedge excision of a well-differentiated invasive squamous cell carcinoma. The defect encompassed the skin and cartilage of the mid and lower helix and antihelix, extending into the concha (Fig. 1).

Defect measuring 1.2 cm following the excision of the invasive squamous cell carcinoma.
In this patient, instead of the full earlobe rotation proposed by Jaber et al., we propose a modified and novel option: dividing the earlobe into two skin flaps. Each flap is then rotated 90° to fill both the anterior and posterior walls of the superior defect, allowing for more mobility compared to preserving the integrity of the earlobe. The superior incised borders were sutured to the conchal incised border. A 4/0 nylon suture was used to attach the skin of the rotated earlobe to the lower side of the defect, and a full-thickness M-plasty was performed during suturing to remove redundant skin. Further specifications of the technique are illustrated in Supplementary Material. The immediate result is shown in Fig. 2. One year later, cicatrization was good with minimal deformity of the auricle. Although the ear appeared smaller, the cosmetic result was favorable, and both the patient and the family were satisfied (Fig. 3).
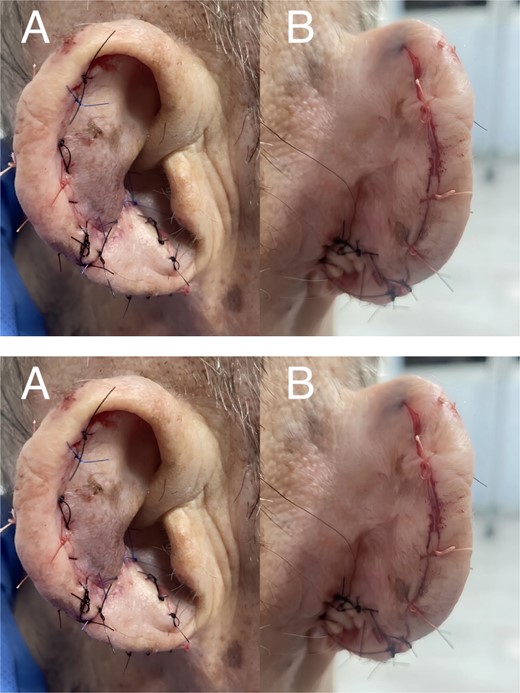
Immediate post-surgical reconstruction: A) Lateral view B) Posterior view.
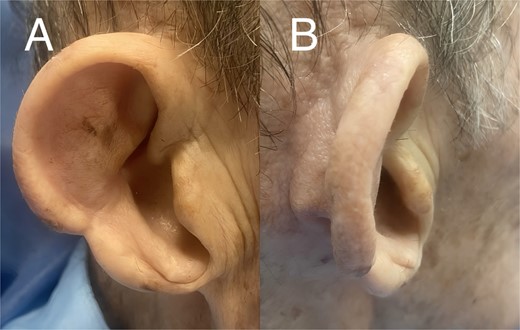
Approximately 1 year after reconstruction: A) Lateral view B) Posterior view.
Discussion
Traditionally, potential one-step repairs after a wedge excision in cases like this include [3]:
1) Wedge excision with direct closure: This technique shortens the auricle while preserving its normal contour. The main limitation is that it is not feasible for wide defects. Additionally, this technique usually causes cupping deformities, except in the smallest cases [2]. Therefore, this technique is typically applicable for defects under 15 mm [4].
2) Full-thickness skin grafts: These may not produce satisfactory results for two-layered auricular defects due to loss of form and stability [3]. Despite its effectiveness, they can lead to partial or total graft failure, warping, color mismatch, and donor site complications [2].
3) Local advancement flaps: These are essential for larger defects in the mid- and antihelix area involving cartilage. Full-thickness resection and reconstruction with Antia-Buch and earlobe flaps result in smaller but esthetically pleasing ears. Advancement and rotation flaps can close full-thickness defects in the mid- and antihelix, with minimal auricular deformity. Antia's chondrocutaneous composite advancement flap, ideal for full-thickness helical rim defects, is suitable only for those in the upper or middle third of the helical rim without extending into the antihelix [2]. Chondrocutaneous advancement flaps are suitable for defects up to 20 mm, and some techniques can repair defects up to 5 cm by combining flaps with wedge excision [4].
Basu et al. proposed in 2013 using the lobe skin as a single skin flap, stating that small local flaps can be raised from the lobe to cover challenging defects in the middle third of the pinna [5]. In 2018, Jaber et al. suggested utilizing the entire lobe and shared their experience with 15 cases. All cases involved adults with keratinocyte cancer and pendulous lobes. They reported favorable outcomes, indicating that all patients healed without complications. This is attributed to the lobule being considered an axial flap richly vascularized. The only deformity observed was the conversion of a pendulous earlobe pattern into an attached one [2].
In conclusion, single-step closures after ear surgery are favored for their cost-effectiveness, reduced morbidity, and fewer hospital visits, making them especially suitable for older adults with limited mobility. We propose a novel modification of Jaber et al.'s earlobe rotation technique by dividing the earlobe into two flaps to enhance mobility. The earlobe, composed of dense connective tissue, serves as a structural component of the ear and, despite lacking cartilage, benefits from rich vascularization, which facilitates excellent healing with minimal complications. Older adults often possess abundant pendulous lobular tissue, which can be utilized for creating cutaneous flaps. The cosmetic outcome is generally satisfactory, as minor asymmetries are rarely a concern given that both lobes are not frequently viewed simultaneously.
Author contributions
ALRV: Conceptualization, supervision, and final review and editing. AML: Data collection, writing, drafting, and editing of the manuscript.
Conflict of interest statement
None declared.
Funding
This work did not receive any funding. The publication charges were covered by the National Autonomous University of Mexico.
Data availability
Data sharing not applicable.
Ethics statement
Written consent for publication was obtained from the patient.

{kind=link}
{kind=link}
{kind=link}