





Abstract
We report the laparoscopic removal of a foreign body that was embedded in the abdominal wall. To the best of our knowledge, this is the first reported case of a foreign body in the abdominal wall being laparoscopically removed. A 27-year-old man working at a forging factory presented to our hospital with abdominal pain. He reported that three hours before presentation, a metal fragment came flying from an operating power hammer and penetrated his lower right abdomen. Abdominal CT revealed a 7 mm-sized radiopaque object near the peritoneum. The foreign body was successfully removed laparoscopically with real-time fluoroscopic guidance. Percutaneous removal is usually performed when a foreign body is present in the soft tissue; however, laparoscopic removal should be considered when the foreign body is located in the abdominal wall near the peritoneum. We provide principles for the safe and minimally invasive removal of foreign bodies based on this case.
Introduction
Patients occasionally present to the emergency room with pain caused by foreign bodies in the soft tissue [1–3]. Although various methods have been reported for the safe and reliable removal of these foreign bodies [2, 4–8], they sometimes fail to effectively remove the foreign body, concerning physicians regarding alternate methods for removal [9]. Here, we report a case of utilizing laparoscopy to remove a foreign body that was embedded in the abdominal wall.
Case report
A 27-year-old man working in a forging factory presented to our hospital with acute abdominal pain. He reported that, 3 hours before presentation, a metal fragment came flying from the operating power hammer, which molded molten metal into the desired shape by striking it. Although he was wearing protective clothing, the fragment penetrated through it and caused sharp pain. Physical examination revealed a 1 cm wound, resembling a stab wound above the right iliac crest (Fig. 1A). The patient experienced localized abdominal pain around the wound; however, there were no signs of peritoneal irritation. His vital signs were stable and laboratory data showed no abnormalities except for a slightly increased C-reactive protein level of 0.91 mg/dL (reference range, 0–0.14). A spine abdominal radiograph showed a 1 cm-sized radiopaque object in the lower right abdomen (Fig. 1B). An abdominal computed tomography revealed a radiopaque object near the peritoneum; however, its exact location being extraperitoneal or intraperitoneal could not be determined (Fig. 2A and B). The abdominal cavity did not have free air or fluid retention. The patient was diagnosed to have a foreign body near the peritoneum and surgical removal was planned. The operation was performed using single-incision plus one-port laparoscopic surgery (SILS plus one). A 1.5 cm longitudinal incision was made at the umbilicus to access the abdominal cavity, after which the wound retractor (Smart Retractor XS; TOP Corp., Tokyo, Japan) was inserted. It was mounted to a single-port access device (Free Access; TOP Corp., Tokyo, Japan). Subsequently a 5-mm trocar was placed just above the pubic symphysis. Laparoscopic inspection following pneumoperitoneum revealed no damage to the peritoneum or internal organs (Fig. 3A). Although we assumed the foreign body was located in the abdominal wall, laparoscopic inspection could not confirm its position. Real-time fluoroscopy was used to locate the fragment. The nearest peritoneum was incised and the abdominal muscle was dissected until the foreign body was observed (Fig. 3B). It was found embedded in the transversus abdominis muscle (Fig. 3C) and was safely removed using forceps (Fig. 3D). The object was 1.5 cm long and sharp at both ends (Fig. 4). The patient was discharged from our hospital after a good postoperative course.
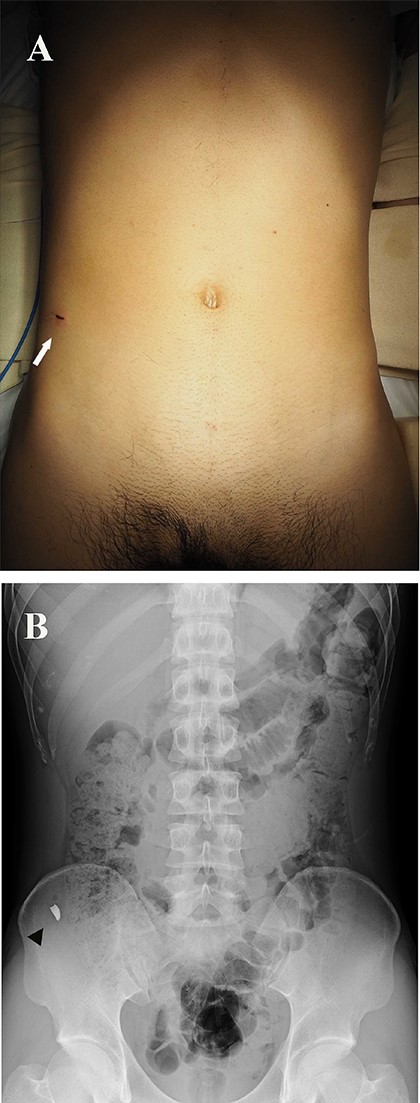
(A) Photograph showing a 1 cm entrance wound, similar in appearance to a stab wound above the right iliac crest (arrow). (B) Spinal abdominal radiograph showing a 1 cm-sized radiopaque object in the lower right abdomen (arrow head).
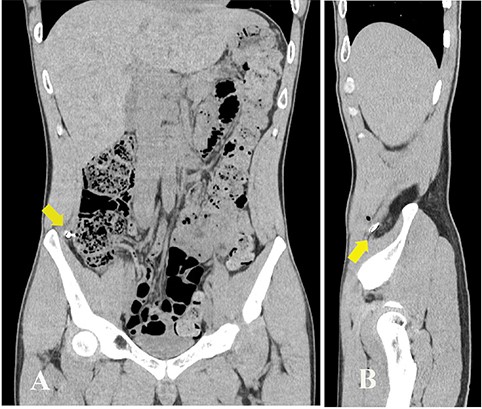
Abdominal CT showing a radiopaque object near the peritoneum. (A) coronal view; (B) sagittal view (arrows).
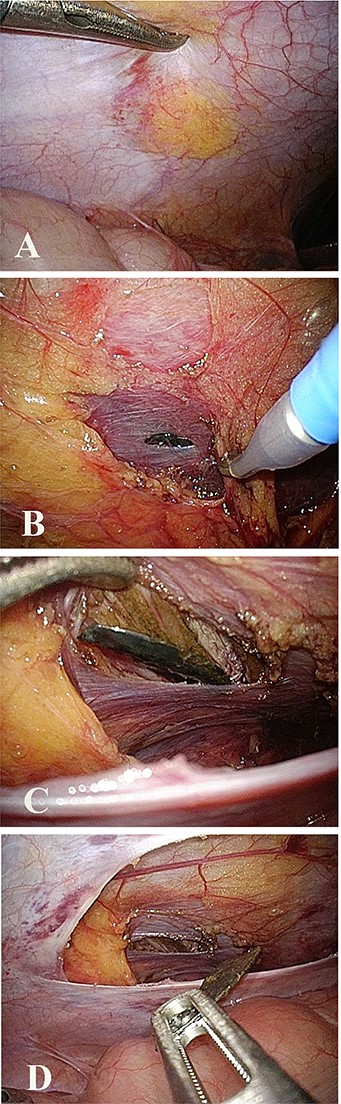
Intraoperative laparoscopic view. (A) No peritoneal damage was confirmed, and the foreign body could not be seen through the peritoneum. (B) Peritoneal incision and muscle dissection made in the area nearest to the foreign body. (C) Foreign body found in the transversus muscle. (D) Foreign body grabbed and removed using forceps.

Photograph showing a foreign body 1.5 cm long and sharp at both ends.
Discussion
Several studies have reported the removal of foreign bodies and various objects have been identified as foreign bodies [1, 3, 4, 7, 10]. These occur in various condition [11]. Projectiles, such as bullets, can become foreign bodies when they strike the human body. While typically associated with battlefields or crime scenes, projectiles can also occur in everyday environments. Similar to our case, metal-processing workplace represent an environment in which projectiles are most likely to be generated [12, 13]. When a foreign body is embedded in soft tissue, percutaneous removal is usually performed under local anesthesia [1, 14]. In general, the deeper the object is, greater is the difficulty in removing it [2].
Key considerations for foreign body removal include:
Confirming the foreign body location using preoperative imaging [2, 3, 5, 6, 9].
Determining the shortest access route that allows minimizing dissection for removing the foreign body [2, 3, 5, 6, 9].
Operating under real-time guidance, as the foreign body location may shift during the procedure [2, 3, 5, 6].
Based on preoperative physical examination, laboratory data, and imaging, we diagnosed the foreign body to be located near the peritoneum with no intra-abdominal organ damage. The patient was a young and muscular man. If percutaneous removal had been performed in our case, postoperative pain caused by skin and muscle damage would have occurred. The abdominal muscle would have disrupted us search and removal. Therefore, under general anesthesia with muscle relaxation, we laparoscopically removed the foreign body from the abdominal cavity side. This approach provided the shortest, least invasive route to the foreign body. Fixing the abdominal wall by the pneumoperitoneum minimized the intraoperative movement of the foreign body during the operative procedure and allowed an excellent view of the peritoneum. We initially assumed that confirming the foreign body location would be simple via laparoscopic inspection. However, it was undetectable through the peritoneum, and no signs of peritoneal damage or hemorrhage were observed to suggest its presence. Probing the peritoneum with forceps was also unsuccessful. We then used fluoroscopy to locate the foreign body via tapping the surface immediately above it. After identifying its position, we then incised the peritoneum and dissected the abdominal muscles to safely remove the object. Consequently, the foreign body was safely removed in a minimally invasive manner. Fortunately, the projectile remained in the transversus abdominis muscle, with no organ damage. To our knowledge, this is the first case report detailing the laparoscopic removal of a foreign body from the abdominal wall.
Conclusion
Thus, we report a case of the laparoscopically removing a metallic foreign body embedded in the abdominal wall. Laparoscopic removal should be considered when foreign bodies are located in the soft tissues of the abdominal wall near the peritoneum. In any case, a device that monitors the location of the foreign body should be used intraoperatively to ensure its safe and secure removal.
Acknowledgement
Portions of this work were presented at the 86th annual Congress of Japan Surgical Association, November 2024, in Tochigi, Japan.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Funding
No funding was received for this case report.
Authorship declaration
All authors agree to the content of this manuscript.
Ethical statement
The patient was informed that data from the research would be submitted for publication, and consent was obtained.

{kind=link}
{kind=link}
{kind=link}
{kind=link}