





Abstract
Bronchogenic cysts, a rare congenital pulmonary disorder, typically affect young adults and are often managed conservatively. However, large cysts with recurrent infections require surgical intervention. This case study highlights the successful management of a large bronchogenic cyst. A 53-year-old female presented with a decade-long history of recurrent respiratory infections manifesting as cough, yellow purulent sputum, and shortness of breath. Chest computed tomography revealed a large bronchogenic cyst in the right middle lobe, causing cardiac compression. Despite conservative management, the recurrent symptoms persisted. After multidisciplinary consultation, a thoracoscopic right middle lobectomy was planned. Severe pleural adhesions and bleeding complicated the procedure; therefore, thoracotomy was performed. Postoperatively, the patient developed transient fever and elevated white blood cell count, both of which resolved with appropriate antibiotic therapy. The patient was discharged in stable condition, with no recurrence of symptoms at follow-up. Large, symptomatic bronchogenic cysts that cause recurrent infections require surgical resection.
Introduction
Pulmonary cystic diseases include lung lesions containing gas or liquid, can be congenital or acquired [1]. Bronchogenic cysts, a type of congenital bronchial developmental disorder, typically affect young adults [2]. They are primarily caused by abnormal budding of part of the bronchial tree [2]. Large cysts may induce respiratory distress, and when infected, bronchogenic cysts often present with high fever and purulent sputum [3]. Differential diagnosis is crucial owing to nonspecific symptoms [4]. Untreated bronchogenic cysts may lead to complications or malignancies [2]. Although most bronchogenic cysts are incidentally discovered during imaging studies, some patients may exhibit symptoms due to infection [3]. The clinical presentation varies widely, with common symptoms including cough, fever, and dyspnea [3]. While bronchogenic cysts are typically managed conservatively, surgical intervention is warranted in cases of recurrent infection [2, 5, 6]. Here, we present a case of a large bronchogenic cyst in the right middle lobe.
Case presentation
History/examination
A 53-year-old female presented with a 10-year history of recurrent cough and purulent sputum. In 2012, chest computed tomography (CT) revealed a cyst in the right middle lobe. Symptoms recurred annually despite antibiotic therapy. Two months prior to admission, the patient experienced another episode of productive cough and fever, accompanied by chest tightness and shortness of breath. A chest CT on 16 January 2024, revealed a giant cyst measuring 8.4 × 7.0 cm in the right lung.
Differential diagnosis, investigations, and treatment
The patient was admitted on 20 March 2024. Enhanced chest CT revealed a solitary cystic lung lesion in the right middle lobe, measuring 8.0 cm × 7.3 cm, with a thin wall and slight compression of the right cardiac border (Fig. 1).
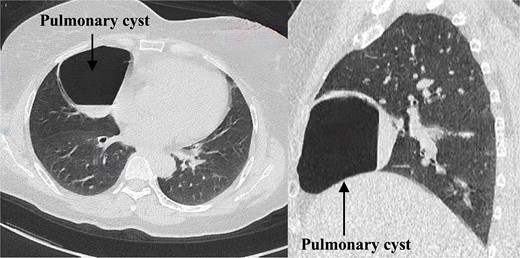
Preoperative enhanced chest computed tomography.
The enhanced scan displayed mild enhancement of the cyst wall without abnormal blood vessels. Pulmonary function tests indicated mild obstructive ventilatory impairment. The patient could ascend 13 floors without stopping during a stair-climbing test. Given the large size of the cyst and a decade of recurrent cough despite conservative treatment, the patient chose surgical intervention. After multidisciplinary consultations, a thoracoscopic right middle lobectomy was planned [7, 8].
Under general anesthesia with double-lumen endotracheal intubation, the patient was positioned in the left lateral decubitus position. A right fifth intercostal anterior-lateral incision was made. Severe pleural adhesions were encountered and carefully separated. The cyst in the right middle lobe (Fig. 2A) was punctured to release pus and gas (Fig. 2B), leading to cyst wall collapse. The puncture site was sutured. While separating the oblique fissure, accidental damage to the pulmonary artery caused bleeding; thus, thoracotomy was performed. The pulmonary artery was repaired (Fig. 2C). The right middle lobe was removed (Fig. 2D). The total intraoperative blood loss was ~500 ml, and the patient received a transfusion.
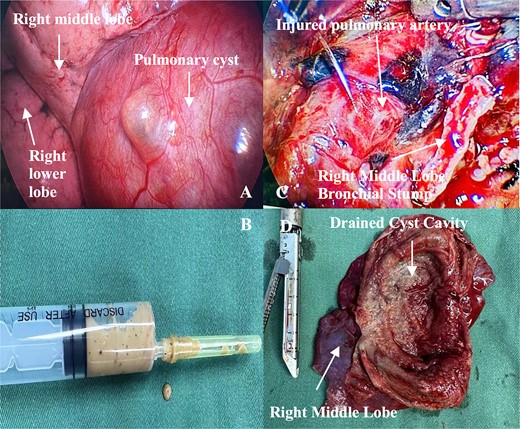
Intraoperative images. (A) Cyst in the right middle lobe and surrounding structures. (B) Pus aspirated from the cyst cavity. (C) Injured pulmonary artery. (D) Resected right middle lobe and opened cyst.
A follow-up chest CT scan 1-month post-surgery showed no pneumothorax, pleural effusion, or pneumonia (Fig. 4). The patient reported no symptoms of cough, sputum production, chest tightness, or shortness of breath and exhibited good daily activity performance.
Postoperatively, the patient began oral intake after 6 hours. On postoperative Day 1, the vital signs of the patient stabilized, and cardiac monitoring was discontinued. A complete blood count indicated elevated white blood cells (WBC count 23.67 × 109/L); however, the body temperature was normal. The patient received intravenous cefuroxime sodium 1.5 g every 12 hours for infection and oral ambroxol for mucus clearance. Coagulation tests indicated a D-dimer level of 9.84 μg/ml, prompting the administration of subcutaneous enoxaparin 4000 U once daily to prevent deep vein thrombosis. The patient began ambulation on postoperative Day 1 under multimodal analgesia. On postoperative Day 2, a fever developed, peaking at 38.1°C with a heart rate of 104 bpm. The patient reported a cough with yellowish sputum. Despite 3 days of cefuroxime sodium treatment, the patient continued to have a fever (37.8°C) and purulent sputum. Therefore, on postoperative Day 4, the antibiotic regimen was switched to intravenous piperacillin–tazobactam 4.5 g every 12 hours. By Day 5, the body temperature normalized. After three days on piperacillin–tazobactam, a repeat complete blood count showed a significant reduction in WBC count (8.89 × 109/L), and antibiotics were discontinued. A chest X-ray on postoperative Day 4 confirmed effective re-expansion of the right lung. Daily drainage volumes were 50–190 ml. The chest drainage tube was removed on postoperative Day 7. Cultures from the intraoperative pus and postoperative sputum did not yield any pathogens, with only normal flora being identified. Pathological examination of the excised right middle lobe confirmed a bronchogenic cyst (Fig. 3). The patient was discharged on Day 9 post-surgery.
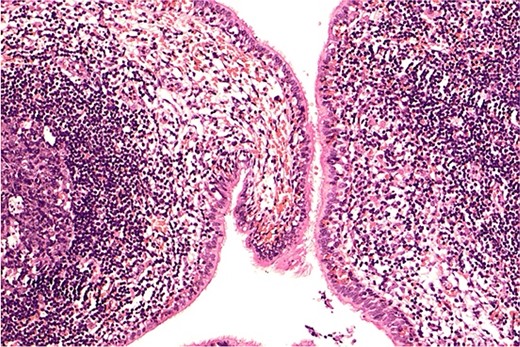
Postoperative paraffin-embedded pathology slide.
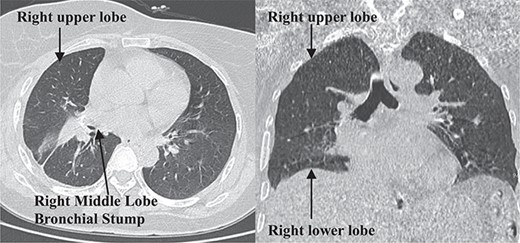
Postoperative 1-month follow-up non-contrast chest computed tomography.
Discussion
This case underscores the potential for early surgical intervention to prevent complications and improve outcomes, particularly in cases where the size of the cyst and symptoms suggest a higher risk [6].
The unpredictable natural course of bronchogenic cysts has led to ongoing debate regarding the optimal management of asymptomatic mediastinal cysts. A previous study reported that early surgical management might be advisable to prevent symptomatic complications, which are unpredictable and more challenging to manage [8]. This aligns with our findings that early intervention could have potentially prevented the complications.
Preoperative respiratory management was critical. An enhanced preoperative chest CT was crucial for identifying variations in pulmonary arterial anatomy, as unrecognized vascular anomalies [9]. Intraoperative findings of significant pleural adhesions and pulmonary artery injury highlight the complexity and risks associated with thoracoscopic resection of large cysts [5, 10]. Conversion to thoracotomy was essential for managing bleeding and removing the cyst safely [11, 12]. The detection of pus within the cyst cavity confirmed recurrent infection, reinforcing the necessity of surgery [4]. Postoperatively, the patient developed transient fever and elevated WBC count, managed with appropriate antibiotic therapy, highlighting the importance of vigilant postoperative monitoring [13]. Ultimately, the symptoms of the patient were fully alleviated, with no recurrence observed during follow-up, validating the efficacy of surgical resection for symptomatic bronchogenic cysts [14, 15]. Early surgical intervention and comprehensive preoperative assessment are crucial for managing large, symptomatic bronchogenic cysts to prevent complications and improve patient outcomes.
Acknowledgements
We thank Dong Yuan for the support provided in revising the manuscript.
Author contributions
X.W. obtained funding. C.T., X.Z., and X.W. designed the study. Q.Q., H.W., X.C., C.T., X.Z., and X.W. contributed to the manuscript writing and assisted in the collection of patient information, image data, and pathological results. Q.Q., H.W., X.C., C.T., X.Z., and X.W. critically revised the manuscript for important intellectual content. Q.Q., H.W., X.C., C.T., X.Z., and X.W. reviewed and approved the final manuscript.
Conflict of interest statement
The authors declare no conflicts of interest.
Funding
This study was supported by the Natural Science Foundation of Sichuan Province (Grant number: 2023NSFSC1047).
Data availability
The data and materials are available from the corresponding authors upon reasonable request.
Ethics approval
This study was conducted in accordance with the Declaration of Helsinki and was granted ethical exemption by the Ethics Committee of Bazhong Hospital of Traditional Chinese Medicine.
Patient consent
Informed consent was obtained from the patient included in the study.
Consent for publication
The patient signed a consent form agreeing to the publication of the data collected during the study.
References
Author notes
Xing Wei, Xiuxiong Zhang, and Chao Tu contributed equally to this work as corresponding authors.

{kind=link}
{kind=link}
{kind=link}
{kind=link}