





Abstract
Intussusception is a phenomenon commonly associated with the paediatric population. In adults, intussusception is frequently a result of a neoplastic process. We present the case of a 56-year-old gentleman who was diagnosed to the local Emergency Department with a 4-day history of worsening severe, left sided lower abdominal pain. The pain was colicky in nature. Computed tomography identified a long-segment intussusception involving distal small bowel, caecum, ascending colon, the entirety of transverse colon and its associated mesentery. The patient proceeded to theatre where a laparotomy and right hemicolectomy was performed. Histopathological analysis of the specimen identified an ileal myxoma as the lead-point of the intussusception. This report emphasises the value of prompt investigation in atypical clinical presentations.
Introduction
Benign tumours of the small bowel are rare clinical phenomena, typically identified in the setting of a complication such as haemorrhage or obstruction [1]. Although rare, adult intussusception is recognised in the literature, often as a consequence of a mass or tumour which serves as a lead point for the intussusception [2]. Although no consensus guidelines exist for the management of Adult Intestinal Intussusception, reduction and resection of the affected bowel based on presumed aetiology is the most widely adopted management approach [3]. This report presents the case of an otherwise well 56-year-old male, seen in the Surgical Assessment Unit of a university with non-specific, episodic abdominal pain.
Case report
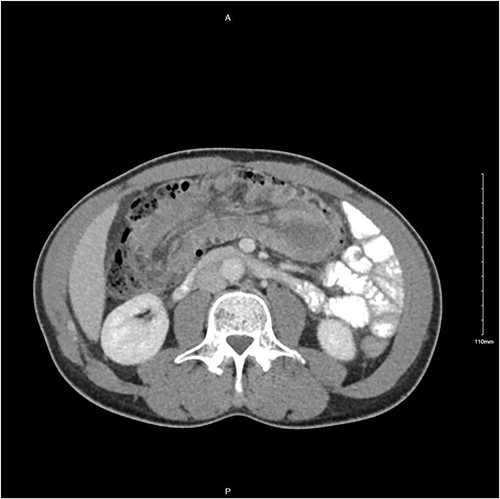
A 56-year-old male was diagnosed with a 4-day history of worsening, cramping left-sided lower abdominal pain and persistent vomiting. The patient had experienced intermittent bouts of similar pain in the previous few months; however, the sustained nature of the pain on this occasion prompted his presentation. Clinical examination elicited lower abdominal tenderness, most marked in the right para-umbilical region. He was an otherwise healthy patient, with no pertinent medical history. Initial investigations revealed a white cell count of 11.78 × 109/L with an associated mild neutrophilia of 9.29 × 109/L. His C-reactive protein was significantly elevated at 130 mg/L, with remaining haematological tests otherwise unremarkable. A computed tomography (CT) scan with intravenous contrast of the abdomen and pelvis was performed which identified a long segment (21 cm) of intussusception involving the distal small bowel, caecum and ascending colon and entirety of transverse colon, including mesentery (Fig. 1). A 5.5-cm hypodense mass was noted within the splenic flexure of the transverse colon which acted as a lead point for intussusception (Fig. 2). There was no pathological small bowel dilatation. Radiologically, the suggested differential diagnosis included gastrointestinal stromal tumour, carcinoid tumour, leiomyosarcoma, lymphoma or benign pathologies such as leiomyoma. The patient proceeded to theatre whereby a formal resection by means of extended right hemicolectomy and primary anastomosis was performed. Histological analysis demonstrated an ileal myxoma to be the causative pathology. The patient had an unremarkable post-operative course and was discharged well 1 week post-operatively.

Transverse CT image of small bowel intussusception into the ascending colon.
Transverse CT image demonstrating long segment of small bowel telescoping towards splenic flexure of the colon.
Discussion
This report details an unusual case of adult intussusception secondary to an ileal myxoma. This patient’s presentation emphasises the value of prompt investigation in cases of diagnostic uncertainty based on clinical history.
Adult Intestinal Intussusception is recognised in the literature as a rare event, with the vast majority of cases having an identifiable cause, be that benign or malignant in nature [3]. Historically, adult intussusception was most commonly diagnosed at the time of surgery; however, with the advent of CT imaging, it is possible to identify cases pre-operatively with remarkable sensitivity. Sonography can also be a very useful diagnostic adjunct in cases where CT may not be readily available [4, 5]. In the case presented in this report, the sub-acute nature of presentation allowed for CT to be performed giving a vastly more detailed peri-operative picture than history alone had suggested.
Although rare, reports of small bowel myxoma in the literature date back as far as 1948, when Stout and colleagues reported five identified cases of small bowel myxoma, one of which involved ileal myxoma with intussusception [6]. Myxomas are invariably benign simple neoplasms of connective tissue, which resemble primitive mesenchyme histologically and are most frequently found in the skin, bony structures or lower genitourinary tract [7].
Given the potential complications of intussusception, prompt evaluation and diagnosis is integral to patient safety, thus ensuring good patient outcomes. This case report demonstrates the invaluable contribution of CT imaging in the diagnoses and surgical planning of this patient.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Funding
No funding was required for this report.

{kind=link}
{kind=link}