





Abstract
Adrenal cysts are rare lesions that make up 4% of all adrenal masses. They are often found incidentally during imaging or surgery and can vary in symptoms depending on their size and location; with cysts < 10 cm often being asymptomatic. These cysts are more common in adults in their 30s or 60s and can be divided into four histological subtypes, with epithelial cysts being less common. We present a case of a 17-year-old female who experienced recurrent right flank pain for a year. Ultrasonography revealed a cystic mass on the right kidney, and computerized tomography showed a well-defined suprarenal cyst measuring ~8 cm misdiagnosed as mesenteric cyst. However, during laparoscopy, an adrenal cyst was discovered, which was excised along with the right adrenal gland. Histopathology confirmed the diagnosis of an epithelial adrenal cyst. This case highlights the occurrence of adrenal cysts in younger individuals and the uncertainty of preoperative diagnosis.
Introduction
Adrenal cysts are rare retroperitoneal lesions that were first reported during an autopsy in 1670 by Greselius. These cysts are often found incidentally comprising only 1%–2% of all adrenal incidentalomas [1]. Most cases are nonfunctional and asymptomatic; however, depending on the size and position of the cysts, clinical manifestations vary from palpable mass, and abdominal pain to more severe gastrointestinal symptoms. They are classified into four types: pseudocysts, epithelial cysts, endothelial cysts, and parasitic cysts, with an average age of diagnosis around 52.3 years [2]. Epithelial or true adrenal cysts are particularly rare representing only 9% of all adrenal cysts [3]. The etiology remains unclear and the diagnosis is confirmed upon histopathological examination as preoperative diagnosis is often complicated with other abdominal masses. We, herein, present a unique case of an epithelial cyst in the right adrenal gland of a 17-year-old female that was initially misdiagnosed as a mesenteric cyst.
Case presentation
A 17-year-old female presented with mild pain in her right flank for the past 4 months. The pain was non-radiating and not associated with nausea or vomiting. The patient had the same complaint a year ago, which was disregarded because of the lack of access to a healthcare center. The pain did not relieve on medication and the patient was referred to our department. On physical examination, the abdomen was soft and non-tender without distention. There was no dysuria, hematuria, or fever. There was no history of weight loss, loss of appetite, or change in bowel movement. The patient had normal puberty, current menstrual cycle is regular and no hirsutism was observed. Patient’s past medical and surgical history was insignificant. Vital signs and blood tests were within normal. Renal/hepatic function panel was within normal range. Abdominal ultrasound showed a large cystic lesion measuring 9 × 9 × 12 cm on the right kidney (Fig. 1). Subsequent abdominal computerized tomography (CT) with contrast showed a large, well-defined, clear fluid-filled suprarenal cyst posterior to the liver, isolated from the liver, right kidney, and the right adrenal gland measuring 8 cm (Fig. 2A–B). Depending on the imaging results which were mistakenly found consistent with a mesenteric cyst, we opted for laparoscopic surgery since the cyst was symptomatic. A surgical exploration of the abdomen revealed an adrenal cyst. The cyst was excised along with the right adrenal gland. Histopathological examination of the resected cyst showed the cystic wall lined by a single layer of cuboidal or flattened epithelium with other sections of normal adrenal cortex tissue, confirming the diagnosis of an epithelial adrenal cyst (Fig. 3). The patient was discharged the next day, her recovery was uneventful and the pain resolved after the removal of the adrenal cyst and did not require further treatment.
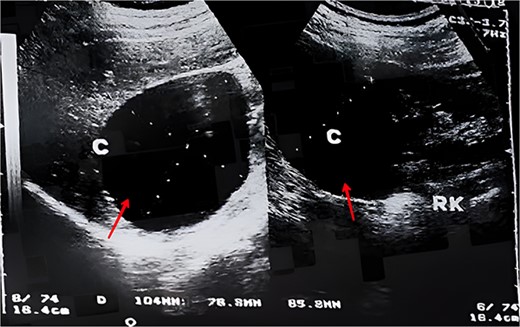
An ultrasonography image showing a cystic mass (arrow) measuring 9 × 9 × 12 cm on the right kidney.
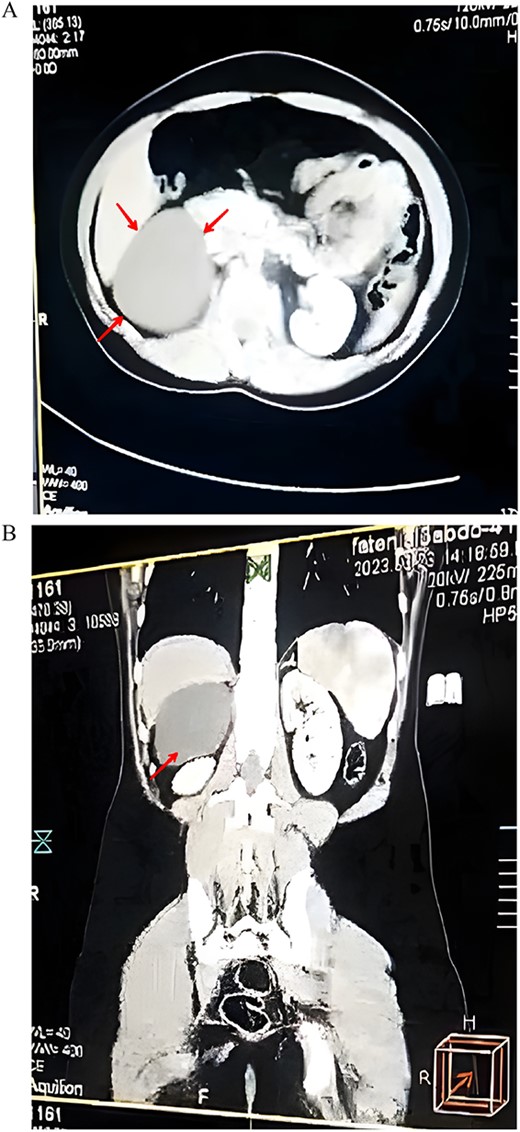
(A) An axial CT scan showing a well-defined suprarenal cyst (arrow). (B) A coronal CT scan of the abdomen showing the location of the cysts in the right upper quadrant (arrow).
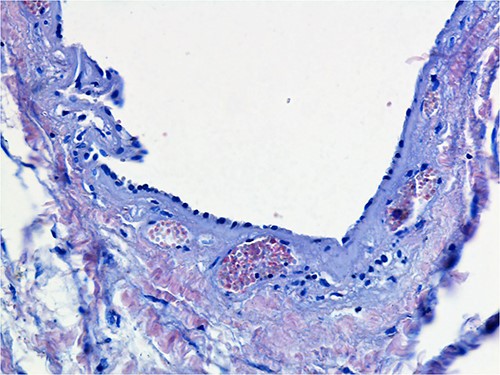
Histopathology shows parts of the cyst’s wall lined by a single layer of cuboidal or flattened epithelium.
Discussion
Adrenal cysts are extremely rare retroperitoneal lesions that account for only 4% of all adrenal masses [4]. They are underrecognized as they present with nonspecific clinical and radiological features. Adrenal cysts are mostly benign and have malignant potential in only 7% of cases [5]. Symptoms vary in presentation according to the size and position of the cyst; smaller cysts are often asymptomatic, nonfunctional, and discovered incidentally. However, larger cysts (>10 cm) are less frequent and are associated with symptoms ranging from abdominal discomfort to more severe presentation complicated with infection, hemorrhage, or rupture [6].
The case presented here involves a relatively small adrenal cyst measuring 8 cm. Nevertheless, the patient experienced recurrent right flank pain for a year, a rarity for cysts of this size to be symptomatic.
Adrenal cysts can occur at any age; however, they are most commonly reported in the third and sixth decades of life and have a slight female predominance [6]. There have been very few reported cases of adrenal cysts in younger people [7, 8], hence, the early presentation in our 17-year-old patient was very uncommon and contributed to the misdiagnosis of the adrenal cyst initially.
Adrenal cysts were classified based on histopathologic features into four types: endothelial cysts (45%), pseudocysts (39%), epithelial cysts (9%), and parasitic cysts (7%) [3]. Our case falls under the category of epithelial cysts, described as true cysts lined by cuboidal to flattened cells with bland cytologic features. In addition to the low incidence rate of epithelial cysts, the few reported cases of epithelial cysts were in older patients. Accordingly, the development of true adrenal cysts in younger people is a rare event, only one study reported a similar case in a slightly older patient aged 25 years [9].
Adrenal cysts are typically diagnosed by CT scan; however, the diagnosis can sometimes be inconclusive. In some cases, this can lead to misdiagnosis when imaging fails to determine the origin of retroperitoneal tumors; therefore, are diagnosed during surgery. A similar case was reported in a 47-year-old patient with a large adrenal cyst misdiagnosed and followed up as pancreatic cystic tumor [10]. Another study reported a case of a giant adrenal cyst diagnosed during surgery [8]. In the case of our patient, the cyst was diagnosed intraoperatively after initially being mistaken for a mesenteric cyst. This emphasizes the uncertainty of preoperative work and failure to establish an accurate diagnosis of adrenal cysts, hence, surgical intervention serves both diagnostic and therapeutic purposes in such cases.
Since adrenal cysts are rare and preoperative diagnosis can be uncertain, there is no established management protocol. However, surgical resection is recommended for: symptomatic cysts regardless of their size, cysts larger than 5 cm and when malignancy is suspected. Laparoscopic adrenalectomy remains the preferred approach, as described in this case, whereas others can be adequately managed with follow-up imaging [9].
To conclude, this unusual case of epithelial adrenal cyst highlights the need to consider adrenal cysts as a possible cause of cystic abdominal lesions, particularly in younger patients, taking into account other common lesions of the adrenal gland such as pheochromocytoma and myelolipoma, which can be ruled out upon Ct findings, whereas, some adrenal cysts are only identified during surgery despite incidental radiological findings. Adrenal cysts are underreported and their underlying causes remain unclear, emphasizing the importance of documenting new cases to further understand this condition.
Conflict of interest statement
All authors confirm that there are no known conflicts of interest associated with this publication and there has been no significant financial support for this work that could have influenced its outcome.
Funding
None declared.
Data availability
All data are available upon request.

{kind=link}
{kind=link}
{kind=link}