





Abstract
Although Meckel’s diverticulum is the most common congenital anomaly of the small bowel (2% prevalence worldwide), it rarely causes symptoms, with only 4% of those with the anomaly developing any complications, including Meckel’s diverticulitis. In contrast to this, appendicitis is the most common general surgical emergency, with a lifetime incidence of 6.7–8.6%. Therefore, the case of a man presenting with right-sided abdominal pain to an Emergency Department with both Meckel’s diverticulitis and appendicitis is rare. This case study illustrates the importance of careful assessment of the entire abdomen when operating on patients with right-sided abdominal pain, so as not to miss Meckel’s diverticulitis even when appendicitis has already been found.
INTRODUCTION
Meckel’s diverticulum (MD) is the commonest congenital gastrointestinal tract anomaly with an incidence of ~2% worldwide [1]. It is a real diverticulum that contains all the layers of the small intestinal wall and results from incomplete obliteration of the omphalomesenteric duct [2]. Although usually asymptomatic, ~4%of people with MD will develop complications such as obstruction, intussusception, bleeding, diverticulitis or perforation and malignancy [3]. Acute Meckel’s diverticulitis is thought to occur secondary to stasis and bacterial infection caused by obstruction of the diverticular neck by enteroliths, foreign bodies, inflammatory tissue, parasites or tumours [4]. Diverticular torsion may also result in ischaemia, and inflammatory change or ulceration of ileal mucosa may occur secondary to acid secretion from ectopic gastric mucosa [5]. If untreated, Meckel’s diverticulitis can lead to perforation and peritonitis. Meanwhile, with a lifetime risk of 6.7–8.6% [6], appendicitis is 100-fold more prevalent than Meckel’s diverticulitis. This case report explores the rare case of a man with both conditions concurrently.
CASE REPORT
A 62-year-old man presented to the emergency department with a 1-day history of worsening right lower abdominal pain associated with nausea and fever. His medical history includes a transurethral resection of the prostate for acinar adenocarcinoma. Clinical examination revealed a soft abdomen with tenderness to palpation at the right lower quadrant. Inflammatory markers showed an elevated white cell count of 12 000/μL and a C-reactive protein of 23 mg/L. Computed tomography (CT) scan demonstrated both an inflamed small bowel diverticulum in the right lower quadrant and mild inflammation of the appendix (Fig. 1). The patient underwent laparoscopy the following day, which revealed a 3 cm inflamed MD adherent to the right anterior abdominal wall with localized peritonitis and a concomitant inflamed appendix (Fig. 2). Laparoscopic appendicectomy and limited small bowel resection with a side-to-side stapled anastomosis were performed simultaneously. Histopathology revealed Meckel’s diverticulitis with ulceration and abscess formation and mild appendicitis. He had an unremarkable recovery in the hospital and remained well on outpatient follow-up 4 weeks later.
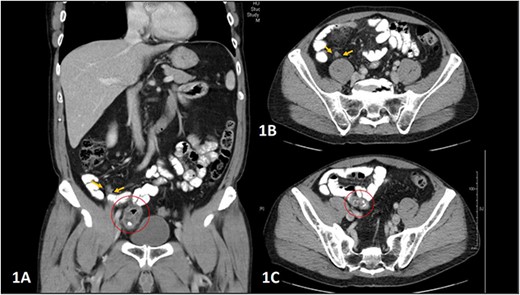
(A–C) Abdominal CT scan showing coronal and axial planes (A and B), indicating the inflamed appendix, highlighted by yellow arrows, and coronal and axial planes (A and C) showing the diverticulum arising from a loop of small bowel extending to the right iliac fossa and right pelvis, highlighted within a red circle.
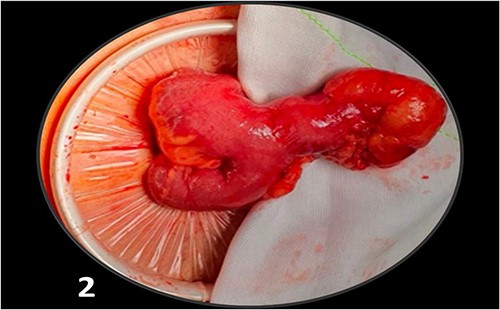
Intraoperative findings include a loop of ileum with a 3 cm blind pouch on the antimesenteric aspect (an MD).
DISCUSSION
MD is the most common congenital anomaly; however, complication of it is rare [1, 3]. Symptomatic MDs are usually managed with segmental bowel resection. In patients with incidentally detected MD on imaging, the evidence does not support elective resection of asymptomatic patients [7]. For those with normal MD found during abdominal surgery, the morbidity associated with resection may be higher than the lifetime risk of Meckel’s-related complications, and the decision to resect needs careful consideration. A selective approach for resection of MD has been suggested based on the presence of risk factors for developing complications, including male sex, younger than 45 years, diverticulum length >2 cm and abnormal features such as a palpable abnormality or fibrous band [8, 9].
Concomitant Meckel’s diverticulitis and acute appendicitis are rarely cited in the literature, and clinically these two conditions can be difficult to differentiate on assessment and imaging alone. Assessment of the small bowel for the presence of MD and its associated complications during laparoscopy for presumed appendicitis should be performed, even if the appendix is grossly abnormal and a diagnosis of acute appendicitis is confirmed. Subsequent resection of MD should be performed if complications such as diverticulitis, perforation or obstruction are evident. Otherwise, a careful evaluation of risk factors should guide decision-making in those with normal-appearing MDs.
Although we had the advantage of preoperative imaging demonstrating dual pathology, we recommend the thorough and careful assessment of the entire abdomen at time of operative investigation of right-sided abdominal pain so as not to miss the rare case of appendicitis with Meckel’s diverticulitis.
ACKNOWLEDGEMENTS
All authors have no personal or financial conflict of interest to declare concerning the research, authorship, and/or publication of this article.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
None.
DATA AVAILABILITY
All data underlying the results are available as part of the article and no additional source data are required.

{kind=link}
{kind=link}