





Abstract
We present a compelling case of disseminated coccidioidomycosis involving the thyroid gland, a remarkably uncommon manifestation of this infection. The gravity of this sporadic disease is underscored by its high mortality rate, primarily because of challenges in timely diagnosis and treatment initiation. Accurate diagnosis hinges upon utilizing various techniques, including the culture of a fine-needle aspirate, biopsy and direct microscopy. However, the medical community is still grappling with the optimal treatment strategy, encompassing considerations such as duration and dosage of medications, which continue to be subjects of intense controversy and ongoing research. This article aims to report an older patient with the incidental diagnosis and management of Coccidioides in the thyroid.
INTRODUCTION
Infection of the thyroid gland with Coccidioides is rare, with fewer than 50 cases reported since 1970. Disseminated infection complicates < 1% of cases and occurs most often in immunocompromised patients. Since most patients are asymptomatic, they may experience a delay in diagnosis and treatment. Fine needle aspiration thyroid biopsy proved helpful in establishing the diagnosis of coccidioidomycosis. The ideal management is unclear, but some studies suggest 3 years of oral azoles after disseminated coccidioidomycosis to other soft tissue organs.
CASE REPORT
An older man was referred for surgical consultation for a suspicious thyroid nodule. His presenting symptomatology was hoarseness and difficulty breathing when supine. The patient did not have dysphagia or odynophagia. He denied weight loss and had no family history of thyroid cancer or any exposure to ionizing radiation.
On physical examination, the patient had a right-sided goiter, a raspy voice and occasional cough. There were no clinically palpable cervical lymph nodes, and cranial nerve examination was unremarkable.
Neck ultrasound demonstrated an enlarged right-sided with a nodule (measuring 3.58 × 4.12 cm) and two left-sided nodules measuring 1.1 and 1.4 cm in size (Fig. 1a and b). The ultrasound also showed a 1 cm nodule inferior to the left lobe, suspicious of a parathyroid adenoma or enlarged lymph node. CT chest revealed multiple nodules in the left pulmonary parenchyma (Fig. 2). Flexible laryngoscopy revealed normal bilateral vocal cord movement but severe inflammation and swelling of the larynx. Subsequent FNA of both the right and left thyroid nodules showed benign results.
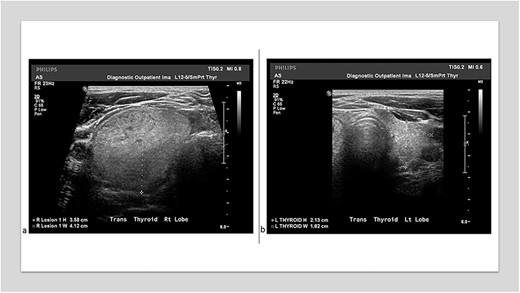
(a) Thyroid ultrasound showed an isoechoic 3.58 × 4.12 cm3 nodule in the right lobe. (b) A thyroid ultrasound showed a left lobe 2.13 × 1.82 cm3.
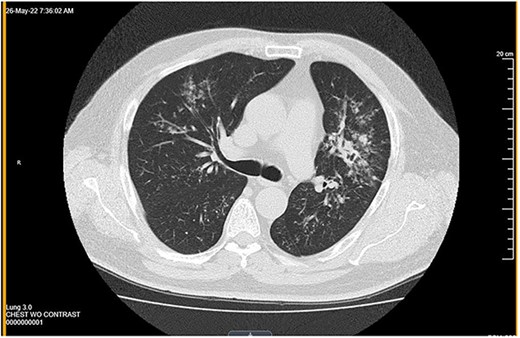
Computed tomography showed multiple nodules in the left pulmonary parenchyma.
An infectious disease specialist evaluated the patient. Sputum culture for acid-fast bacilli (AFB) was negative but was positive for mold compatible with coccidioidomycosis. Mycobacterium tuberculosis complex polymerase chain reaction was negative. Serology testing showed elevated coccidioidomycosis antibody titers (1512, normal range < 1.2).
The patient underwent an uncomplicated thyroidectomy. Histopathologic examination demonstrated a thyroid (108 grams) with nodular and hyperplastic thyroid follicles. Several small nodules in the right lobe consisted of caseating and noncaseating granulomas (Fig. 3a) with spherules (10–40 μm) characteristic of Coccidioides immitis (Fig. 3b and c). No neoplasm was present in any of the tissue. Pathology was negative for acid-fast stain for Mycobacterium. Subsequent CT of the chest showed extensive bilateral miliary nodules. The patient was started on oral fluconazole therapy at 400 mg/d.
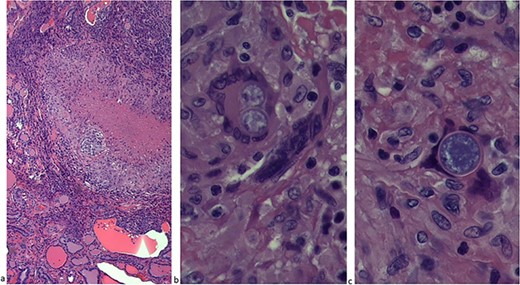
(a) The thyroid lobe consisted of caseating and noncaseating granulomas. (b) Thyroid lobe with spherules (10–40 μm). (c) C. immitis.
The patient had an uneventful recovery status post thyroidectomy. The patient experienced significant improvement in his cough after initiating antifungal treatment.
DIFFERENTIAL DIAGNOSIS
Fungal infections of the thyroid are uncommon. Although the patient did not have pain, a differential diagnosis is the subacute granulomatous thyroiditis, an inflammatory thyroid disorder characterized by a cellular smear with clustered epithelioid cells, fibrous fragments with enmeshed inflammatory cells, scattered lymphocytes, histiocytes and neutrophils, occasional multinucleated giant cells. Moreover, chronic lymphocytic (Hashimoto) thyroiditis is a differential diagnosis because it is a diffuse, non-tender thyroid gland with primary features of oncocytic epithelium, lymphocytes and germinal centers, which lack follicle destruction and giant cells. Another suspect disease was tuberculosis, characterized by granulomas with caseation granulation tissue and fibrosis with an AFB positive. The possibility of sarcoidosis was also raised because of the presence of granulomas with small, compact aggregates of epithelioid histiocytes and giant cells may be present. Necrosis tends to be absent.
DISCUSSION
Thyroiditis caused by C. immitis can be difficult rot diagnose as most patients are asymptomatic. Fungal thyroiditis is generally diagnosed postmortem. Huntington et al. reported thyroid involvement in nine patients out of 130 (7%) postmortem without clinical thyroid dysfunction. The antemortem diagnosis of fungal thyroiditis is led by direct microscopy and culture of a fine-needle aspirate or biopsy [1]. Our patient underwent thyroidectomy because of a sizeable symptomatic goiter, and the histopathology reported the incidental finding of fungal thyroiditis. In the literature, only five patients have reported antemortem [2].
In contrast to most other organs in the body, the thyroid gland is remarkably resistant to infection because of the rich blood supply and lymphatic drainage from the thyroid. Signs and symptoms of the disease include fever, anterior cervical pain, thyroid enlargement sometimes associated with dysphagia and dysphonia, and clinical and laboratory features of transient hyperthyroidism followed by residual hypothyroidism [3]. Our patient presented with a multinodular goiter associated with hoarseness and difficulty breathing when lying down.
The duration of therapy for disseminated thyroid coccidioidomycosis is controversial. Some recommend high-dose daily fluconazole (600–800 mg daily based on tolerance) for up to 36 months of treatment. Other studies support using isavuconazonium as the most effective and least toxic azole in refractory patients [4]. Also, some patients required surgery for adjunctive or definitive treatment.
Additionally, since differentiating fungal thyroiditis from subacute thyroiditis is difficult, corticosteroids can increase fungal infection locally and systemically [5].
CONCLUSION
This case report discusses a rare occurrence of disseminated coccidioidomycosis in the thyroid gland, which presents a significant diagnostic challenge. The disease has a high mortality rate because of diagnosis and treatment initiation delays. Accurate diagnosis requires various techniques, but the optimal treatment strategy remains controversial and is under ongoing research. The article highlights the importance of recognizing and managing Coccidioides infection in the thyroid, particularly in older patients, to improve outcomes and reduce mortality rates.
AUTHORS’ CONTRIBUTIONS
Paola Solis-Pazmino and Eyas Alkhalili: conceived and designed the work. Paola Solis-Pazmino and Natalie Merchant: drafted the manuscript. Osvaldo Padilla: images collection. Paola Solis-Pazmino and Eyas Alkhalili: corrections and final article review. All authors read and approved the final manuscript version to be published.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
The authors declare that no funds, grants or other support was received during the preparation of this manuscript.
CONSENT TO PARTICIPATE
Informed consent was obtained from the patient.
ETHICAL STANDARDS
All procedures followed were by the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
INFORMED CONSENT
Informed consent was obtained from the patient to be included in the study.

{kind=link}
{kind=link}
{kind=link}