





Abstract
Hibernomas are rare and benign lipomatous tumors which consist of lobules of cells derived from brown fat. Less than 200 overall cases are reported in the literature which necessitates the need to report more cases for better understanding of this neoplasm. Hibernomas are slowly progressing, painless tumors most frequently located in the subcutaneous thigh, upper trunk, and neck. Hibernomas generally occur in areas close to the axial skeleton where brown fat used to exist in the fetus and persisted during adulthood. They are rare to be discovered for the first time in older adults, most commonly presenting in adults 20–40 years of age. Core biopsies are simple to perform under local anesthetic and provide pathological differentiation prior to planned excision, hence are recommended, especially with larger lesions. Based on case presentation, watchful waiting for non-growing asymptomatic cases of hibernoma is possible, but more frequent follow-up and/or a core biopsy would be advised to rule out a more aggressive diagnosis. Compared with lipoma-like hibernomas, atypical lipomatous tumor/well-differentiated liposarcoma recurs and might dedifferentiate to a dedifferentiated liposarcoma with the ability to metastasize in up to 5% of the recurrences. Hibernomas, including the lipoma-like variant, are typically treated by surgical excision, rarely recur and do not metastasize. We report two rare presentations of hibernoma and lipoma-like hibernoma. Awareness of this clinicopathological entity is crucial to avoid misdiagnosis as malignant lipomatous neoplasm.
INTRODUCTION
Hibernomas are rare and benign lipomatous tumors which consists of lobules of cells derived from brown fat [1]. Less than 200 overall cases are reported in the literature which necessitates the need to report more cases for better understanding of this neoplasm [2]. Hibernomas are slowly progressing, painless tumors most frequently located in the subcutaneous thigh, upper trunk and neck [3]. Hibernomas generally occur in areas close to the axial skeleton where brown fat used to exist in the fetus and persisted during adulthood [4]. They are rare to be discovered for this first time in older adults, most commonly presenting in adults 20–40 years of age [5]. Treatment consists of surgical excision and rarely recurs after excision [5]. Morphologic variants include lipoma-like hibernoma, myxoid variant and spindle cell variants [2]. Unlike conventional lipomas, hibernomas have granular eosinophilic cytoplasm and multivacuolated cells with numerous lipid droplets [6]. In addition, they have small and bland central nuclei with rare mitotic figures or atypia [1]. Lipoma-like hibernomas consist of mostly mature univacuolated adipocytes with sparse eosinophilic granular and few multivacuolated brown fat cells [6, 7]. Some differential diagnoses of hibernoma include conventional lipoma, lipoblastoma, atypical lipomatous tumor, dedifferentiated liposarcoma, spindle cell/pleomorphic lipoma, myxoid/round cell liposarcoma and pleomorphic liposarcoma among others [8, 9].
CASE PRESENTATION
Case 1
A 32-year-old female presented to the clinic with a palpable soft tissue back mass noticed a month prior to her visit. The patient had not noticed any change in size. On physical examination, a minimally mobile painless soft tissue mass was palpated and located on the left side of the back. No skin changes were noted. The mass was ~13 × 15 cm on palpation. No punctate, drainage nor erythema were noted. The mass was not attached to the skin. Ultrasound was performed 20 days prior to her visit and detailed a large soft tissue mass at the site of clinical concern in the patient’s back on the left side measuring 10.5 × 8.5 × 3.3 cm. Ultrasound-guided core biopsy was performed under local anesthetic in the office setting and demonstrated a Lobulated tumor composed of a mixture of cell types in varying proportions with small, bland, central nuclei, polygonal cells with granular eosinophilic cytoplasm and multivacuolated cells with numerous lipid droplets. Some univacuolated adipocytes were identified. Medium-sized prominent stromal vessels were noticed. Mitotic figures were rare. A computed tomography (CT) scan of chest with contrast was performed to estimate the relationship of the mass to adjacent anatomical structures. The CT scan showed 12.6 × 10 × 3.9 cm lipomatous mass beneath the latissimus dorsi muscle along posterolateral aspect of upper abdomen/lower thorax favoring an intramuscular lipoma (Fig. 3). Patient agreed to have complete excision of the mass. After excision in the operating room, the specimen was sent to pathology and showed a well-circumscribed 266 gm fatty mass that was serially sectioned revealing homogenous yellow adipose tissue on cut section (Fig. 2). The specimen was submitted per grossing protocol which is one section per 1 cm. Final pathology confirmed diagnosis of hibernoma (Fig. 1).
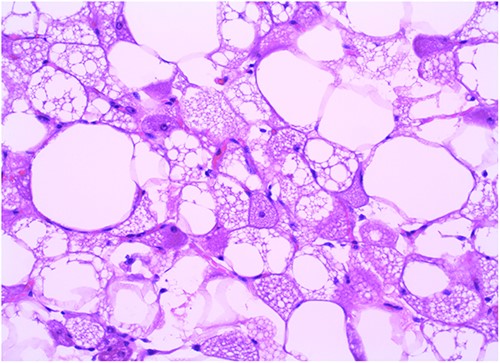
Case 1: hematoxylin and eosin ×20.
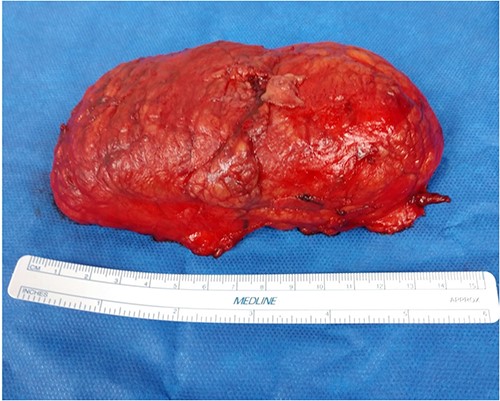
Case 1: gross picture of lesion postoperatively.
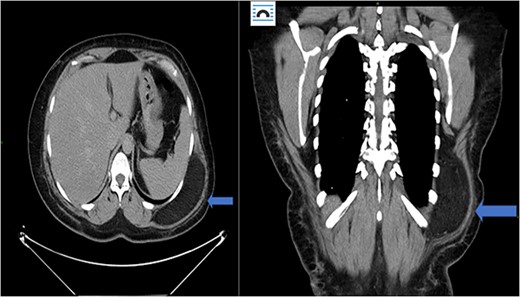
Case 1: CT (axial and coronal view), blue arrow marks hibernoma.
Case 2
A 58-year-old male patient with a medical history of hypertension, type 2 diabetes mellitus, neuropathy and multiple kidney stones presents to the emergency department with complaints of dysuria, frequency of micturition and urgency for the past 4 days. Patient denied any fever. He also described a sharp shooting pain sensation along his left leg that was intermittent and associated with movement. He elaborated that it felt like it mimicked the chronic neuropathy pain which the patient was used to having, but the pain would begin after ambulating for a short distance, such as across a room. It was incapacitating. He denied any recent trauma.
In the emergency department, vital signs were remarkable for elevated blood pressure of 166/81, but otherwise stable and afebrile. WBC count was elevated at 15.4 with left shift and hemoglobin was low at 9.6. Complete Metabolic Panel was notable for hyponatremia of 128, and mildly elevated BUN/serum creatinine of 26/1.5 which was slightly higher than his baseline of 17/1.3. Liver function tests were unremarkable. UA showed likely UTI with positive esterase, high RBC/WBC and bacteria and protein. A CT of the abdomen and pelvis was done, showing a left non-obstructing kidney stone and a left retroperitoneal fat density with stranding along the left iliopsoas measuring 12.6 × 8.1 cm × 3.7 cm, which was described as possibly a part of infectious or malignant process (Fig. 5). Subsequently, patient’s prior CT scans were available to be reviewed and it showed the same lipomatous mass 9 years earlier. (Fig. 6). Given the patient’s symptoms of left lower extremity pain and the possibility that the mass was responsible, a CT-guided core biopsy was ordered for diagnosis to rule out a malignant process as operative intervention was being contemplated. Pathology report of the core biopsy showed lobules of univacuolated adipocytes divided by thin septa. There were frequent multivacuolated adipocytes with small round nuclei, reminiscent of brown fat cells. No enlarged hyperchromatic cells, mitotic figures nor necrosis are seen. The findings supported the diagnosis of the lipoma variant of hibernoma (Fig. 4). Given the chronicity of the mass, the near identical size over 9 years and the diagnosis made from core biopsy, it was determined that the hibernoma was not the likely source of the patient’s LLE pain and hence the mass was not excised.
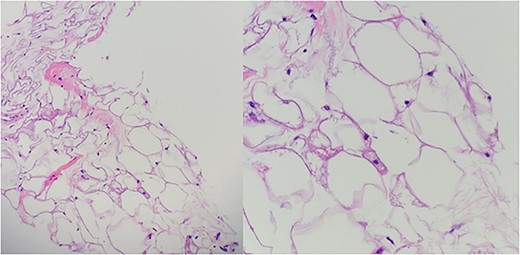
Case 2: hematoxylin and eosin.
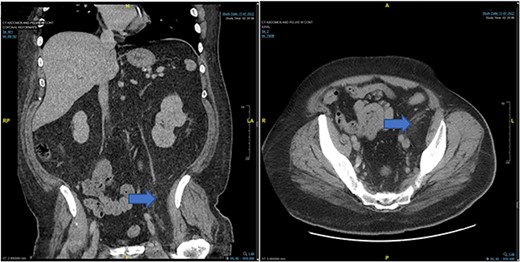
Case 2: CT abdomen and pelvis from November 2022.
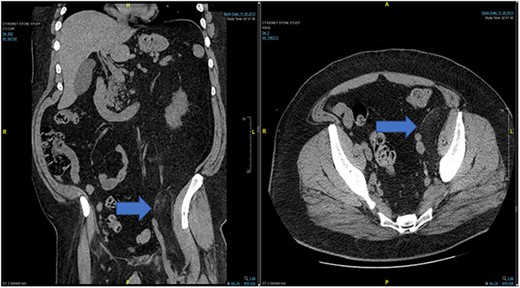
Case 2: prior CT of Case 2 from 2013.
DISCUSSION
Hibernomas are rare and benign lipomatous tumors with differentiation toward brown fat [1]. Brown fat is commonly found in hibernating animals and newborns and is involved in metabolism and thermogenesis regulation [10]. From infancy to adulthood, brown fat is replaced by white fat, with persistence of brown fat in adults most common over the neck, interscapular area, axilla and retroperitoneum [10]. The term hibernoma in fact comes from reasoning that the brown fat cells of hibernomas resemble the brown fat in hibernating species [2]. They are asymptomatic, most commonly presenting as a slowly growing, painless, palpable and soft mobile mass, or as an incidental finding on imaging [11]. Surgical excision is the most common definitive treatment [3]. A few morphologic variants have been identified including lipoma-like hibernoma, spindle cell and myxoid variants [6].
The diagnostic criteria for hibernomas include a circumscribed, lobulated, grossly yellow-brown mass with cellular features of brown fat, including numerous small cytoplasmic vacuoles and eosinophilic granular cytoplasm [6, 9]. Hibernomas are polygonal cytologically bland cells with small and central nuclei, prominent nucleoli, with rare cytologic atypia and mitotic figures [6]. The conventional lipoma in contrast to hibernomas are tumors with differentiation toward white fat cells [12]. The lipoma-like hibernoma variant has copious amounts of univacuolated cells mixed with scattered few granular multivacuolated hibernoma brown fat-like cells [8].
Immunohistochemistry profile in support of hibernomas includes focal positivity of S100 in up to 85% of cases, positive CD 68 and negative CD34 unless combined with a spindle cell lipoma [3]. It is important to distinguish hibernomas, especially the lipoma-like hibernomas from atypical lipomatous tumor/well-differentiated liposarcoma [8]. Lipoma-like hibernomas can appear like the well-differentiated liposarcoma due to the presence of multivacuolated adipocytic cells mimicking lipoblasts in well-differentiated liposarcoma [8]. They can be distinguished by performing immunostains and in situ hybridization for MDM2 [13]. In general, a negative MDM2, negative CDK4 and positive or variable p16 markers may help to distinguish hibernomas from other lipomatous tumors including atypical lipomatous tumor/well-differentiated liposarcoma, dedifferentiated liposarcoma, and spindle cell/pleomorphic lipoma [3].
It is important to be aware of the lipoma-like hibernoma variant to avoid misdiagnosis and extreme treatment [1]. Compared with lipoma-like hibernomas, atypical lipomatous tumor/well-differentiated liposarcoma recurs and might dedifferentiate to a dedifferentiated liposarcoma with the ability to metastasize in up to 5% of the recurrences [8]. Hibernomas, including the lipoma-like variant, are typically treated by surgical excision. They rarely recur and do not metastasize [11]. Since the surgical excision of a benign and malignant tumor varies, a core biopsy is recommended prior to definitive excision to rule out the malignant potential neoplasms.
Morphological differential diagnosis includes the following: normal brown fat which is more abundant in children and young adults than older adults and usually found in neck, axilla, mediastinum and paraspinal regions but no discrete mass lesion should be identified on physical exam [14]. Lipoblastoma may contain brown fat cells and usually occur in infants (<3 years of age). It is characterized by prominent lobularity with myxoid stroma and lipoblasts and can be confirmed by PLAG1 gene rearrangements [15]. Atypical Lipomatous Tumor/Well-Differentiated Liposarcoma have atypical ‘smudge’ cells in thickened fibrous septa. True lipoblasts with hyperchromatic scalloped nuclei may be present. MDM2 amplification is identified by FISH [5]. Granular cell tumors have diffused cytoplasmic granularity, with no multivacuolated cells present, and diffuse S100 protein (+), which is confirmed by immunohistochemistry [16]. Myxoid liposarcoma has a plexiform vascular pattern, with lipoblasts commonly present and hibernoma-like cells uncommon. It also has characteristic t(12;16) or t(12;22). Adult rhabdomyoma has large polygonal cells with abundant eosinophilic cytoplasm. Cytoplasmic cross striations and spider cells may be present; the cells are Desmin (+), myogenin (+) and S100 protein (−) [17]. Chondroid lipoma consists of cellular clusters and nodules of vacuolated cells with conspicuous chondromyxoid or hyalinized stroma [18, 19].
CONCLUSION
Hibernomas are rare and benign lipomatous tumors made up of lobules of cells derived from brown fat. Less than 200 overall cases are reported in the literature. Hibernomas are slowly progressing, painless tumors most frequently located in the subcutaneous thigh, upper trunk and neck, as evident in the two cases presented in this article, they may present anywhere. It is important to be aware of the lipoma-like hibernoma variant to avoid misdiagnosis and extreme treatment. Core biopsies are simple to perform under local anesthetic and provide pathological differentiation prior to planned excision, hence are recommended, especially with larger lesions. Based on case presentation [2], watchful waiting for non-growing asymptomatic cases of hibernoma is possible, but more frequent follow-up and/or a core biopsy would be advised to rule out a more aggressive diagnosis. Compared with lipoma-like hibernomas, atypical lipomatous tumor/well-differentiated liposarcoma recurs and might dedifferentiate to a dedifferentiated liposarcoma with the ability to metastasize in up to 5% of the recurrences. Hibernomas, including the lipoma-like variant, are typically treated by surgical excision, rarely recur and do not metastasize. We reported two rare presentations of hibernoma and lipoma-like hibernoma. Awareness of this clinicopathological entity is crucial to avoid misdiagnosis as malignant lipomatous neoplasm.
DISCLAIMER
This research was supported (in whole or in part) by HCA Healthcare and/or HCA Healthcare-affiliated entities. The views presented in this article represent those of the authors of the article and do not necessarily represent the official views of HCA Healthcare or any of its affiliated entities.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
None.
DATA AVAILABILITY
Data is de-identified and released with permission.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}