





Abstract
In the absence of the mandibular first molar, there is corresponding supra-eruption of the maxillary first molar, which can lead to occlusal interferences compromising the space available for restoration with a prosthesis. In this case report, the maxillary left first molar intrusion has been discussed with the use of two miniscrews. A 28-year-old female reported with a missing mandibular left first molar and wanting to replace it with a dental implant. The patient presented with a Class I skeletal relation, mild proclination of the anteriors and occlusal contacts. The maxillary first molar had erupted by >4 mm beyond the occlusal plane, thereby reducing the space available for placement of a lower prosthetic crown. After 5 months of intrusion, the desired occlusal clearance was achieved, and impressions were recorded. For retention, the patient was given an upper clear vacuum retainer and the crown was placed on the implant.
INTRODUCTION
In the absence of the mandibular first molar, there is corresponding supra-eruption of the maxillary first molar. This may lead to occlusal interferences, periodontal problems as well as mesial inclination of the mandibular second molar, thereby compromising the space available for restoration with a prosthesis [1]. Some of the options for replacing the mandibular first molar are: occlusal reduction of the opposing tooth, aligners, intrusion using appliances or miniscrews or the use of continuous arch-wire mechanics [2]. In such cases, orthodontics is mostly an adjunctive option, with the emphasis of the treatment being the correction of the position of the supra-erupted teeth [3]. Care must be taken to ensure that the desired movement is achieved without any major movements across the rest of the dentition [4].
CASE REPORT
A 28-year-old female reported to the University of Puthisastra’s dental clinic with a missing mandibular left first molar and wanting to replace it with a dental implant. There was minimal mesial inclination of the mandibular second molar, but the prolonged presence of a decayed tooth with decreased clinical height allowed the opposing first molar to extrude. The first option given to the patient was the placement of an implant to replace the missing mandibular molar and occlusal reduction of the maxillary molar to gain space; but on clinical examination, the amount of occlusal reduction required was too much, therefore it was decided to intrude the maxillary molar to gain space for the prosthetic crown.
DIAGNOSIS
The patient presented with a Class I skeletal relation, mild proclination of the anteriors and occlusal contacts. On examination, she was found to have a normal overjet, crowding in the maxillary arch, supra-erupted maxillary left first molar and missing mandibular first and third molars. The maxillary first molar had supra-erupted by >4 mm beyond the occlusal plane, thereby reducing the space available for placement of a lower prosthetic crown.
PLANNED MOLAR INTRUSION
Orthodontic miniscrews measuring 1.6 mm in width and 8 mm in length, respectively, were placed. The screw on the buccal aspect was placed between the maxillary first molar and second premolar, and the one on the palatal aspect was placed between the first and the second molar (Fig. 1). The placement of the screws was planned in order to have a diagonal coverage of the occlusally directed forces for intrusion.
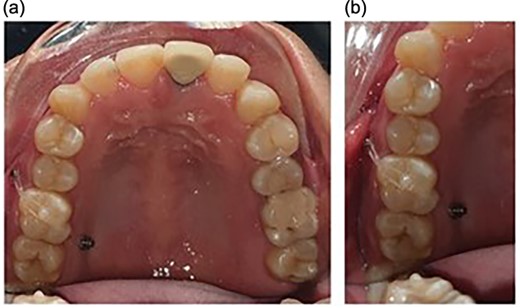
Placement of the miniscrews: (a) on the buccal side between the second premolar and the first molar and (b) on the palatal side between the first and the second molars; composite button on the occlusal surface to direct the forces along the long axis.
Following the placement of miniscrews, immediate loading was done with 100 g of intrusive force using a short power chain. The power chain was passed and engaged onto the composite button to ensure the forces are directed occlusally and there is no slippage. The patient was followed up at 4-week intervals and the power chain was replaced with one link, which was reduced at each appointment. After the first month, the dental implant was placed to replace the mandibular first molar. After 5 months of intrusion, the desired occlusal clearance was achieved and the upper and lower impressions were recorded (Fig. 2). For retention in the upper arch, the patient was given a clear vacuum retainer, while the crown was placed on the implant to prevent any relapse and to achieve good occlusion.

The intrusion process with placement of the prosthetic crown at the completion stage.
RESULTS
The following movements were seen as a result of the intrusion process:
Intrusion of the maxillary left first molar without the requirement of any occlusal trimming or fixed orthodontic appliance.
Slight lingual inclination of the molar because of the length of the elastic chain being more on the palatal side.
Maxillary molar intrusion 4 mm above the occlusal plane (Fig. 3).
Panoramic radiographs recorded at regular intervals showed that the lamina dura around the molar was intact and no root resorption was observed.
Allowed for placement of full coverage crown on the implant placed to replace the mandibular first molar (Fig. 4).
Cephalometric superimposition demonstrated maxillary first molar intrusion without any adverse effects on the inclination of the anterior teeth (Fig. 5).

Panoramic radiographs show the intrusion process along with placement of the implant in the opposing arch.

Full coverage crown placed on the implant to replace the mandibular first molar.
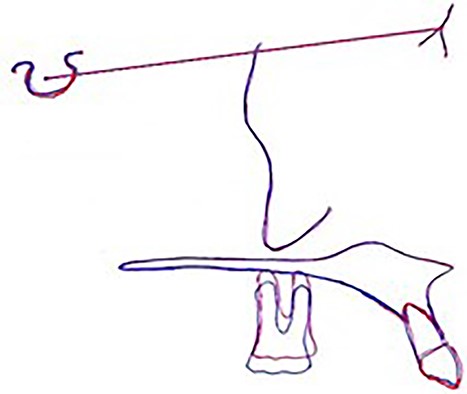
The cephalometric super-imposition denoting intrusion.
DISCUSSION
In this case, the miniscrew was placed between the second premolar and the first molar in the buccal dento-alveolar region, while the second was placed between the maxillary first and second molars. Previously published cases have mostly placed the buccal miniscrew distal to the maxillary molar and the palatal miniscrew mesial to it. Since the inter-radicular bone is sufficient mesial to the maxillary molar, it was decided to place the buccal screw at the level of the muco-gingival junction in the dento-alveolar region. The palatal screw was placed between the two molars, avoiding the greater palatine foramen. In order to prevent any anchorage failure because of the thin nature of bone in that area, the length of the screw utilized was 8 mm. As can be seen from the figures, the miniscrews were placed mesial and distal to the molar to minimize the need for any additional attachments to intrude the molar.
The amount of intrusion achieved was easily comparable with previously published case reports [5]. Different forces were used for molar intrusion in various published articles, but, in this case, we decided to use 100 g of force for intrusion as previous reports have suggested [6, 7].
Previous cases have utilized an elastic separator to open space for intrusion, but, here, it was decided against placing separators to minimize the risk of periodontal damage [8]. In this case, the composite button was not only used to avoid any undesired rolling of the chain but also to deliver forces along the long axis to achieve the best possible results.
From the panoramic radiographs, it can be visualized that there was no observable resorption and the molar easily intruded into the floor of the nasal cavity without any resorption [9]. To minimize the possibility of relapse, the patient was delivered clear vacuum formed retainers for the upper arch while the opposing tooth would receive a full coverage crown on the implant to achieve good occlusion.
CONCLUSION
From the results of this report, it can be seen that maxillary molar intrusion into the nasal floor can be achieved without resorption as long as light continuous intrusive forces are delivered directionally along the long axis of the tooth.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
No funding was received.
DATA AVAILABILITY
The author states that any data related to the treatment carried out will be provided upon request.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}