





Abstract
Vesical calculus is a common condition with familiar aetiology in our environment as it is obtained in other parts of the world. Notwithstanding, uncommon aetiology of this pathology still exists though rarely encountered especially where out-of-pocket payment is the norm for accessing health care services. This is a report of three patients with varying indications for indwelling vesical catheter insertion via urethral or suprapubic route and who developed vesical calculus from prolonged and neglected indwelling vesical catheter. These cases are indeed an enigma in contemporary surgical patient care. We share our experience in the care of these patients and to underscore the extra role expected of health care providers in adequate patient education, close attention to guidance and counseling during patients’ visits to health facilities.
INTRODUCTION
Vesical calculus is a well-known pathology with varying causes commonly resulting from foreign bodies, obstruction or infection [1]. It accounts for 5% of urinary stones and 6.7% of bladder diseases seen in our practice annually [1, 2]. In contemporary times with increased awareness and patient education, it is rare to find the vesical calculus from avoidable aetiology such as a prolonged and neglected indwelling catheter. Several reasons in the healthcare delivery chain ranging from patient poor socioeconomic status, healthcare personnel-related factors to disregard for counseling may play a vital role. Duration of an indwelling urinary catheter is also important. Long-term indwelling catheter lasting longer than a month can be attended to with complications such as bacteriuria, UTI, blockage and bladder stone formation [3]. Therefore, it is recommended that urethral and suprapubic cystostomy catheters be replaced at regular intervals.
Once a significant stone burden is established around an indwelling catheter, non-invasive removal using chemolysis presents an enormous task. The various notable methods of vesical calculus treatment include extracorporeal shock waves lithotripsy, transurethral cystolithotripsy, percutaneous cystolithotripsy, laparoscopic approach, combined percutaneous approach and transurethral cystolithotripsy, transurethral cystolitholapaxy and cystolithotomy depending on the available facilities [4].
CASE REPORT
The first case was a 37-year-old artisan who presented to our facility in the year 2022 with a history of lower urinary tract symptoms that culminated in acute urine retention. The attempt at urethral catheterization failed warranting suprapubic cystostomy. He had past purulent post-gonococcal urethritis which was poorly treated. The Retrograde urethrocystogram confirms incomplete bulbar stricture. There was no other remarkable medical history.
The physical examination was unremarkable and vital signs were within normal range. The laboratory investigations were unremarkable. He was counseled for monthly change of SPC catheter but returned to follow-up clinic after 3 months of suprapubic cystostomy. At this point, the change of SPC was difficult. Transabdominal Ultrasound scan of the abdomen shows hyperechoic appearance at the region of the suprapubic catheter balloon but no definite posterior acoustic shadowing. He had local infiltration of 1% lidocaine injection at the suprapubic region adjacent SPC stoma with successful removal of the suprapubic catheter as shown in Fig. 1B.
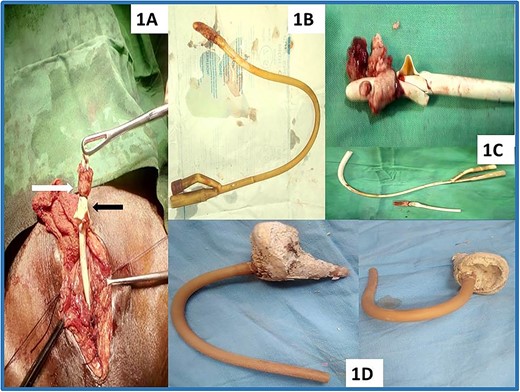
Vesical calculi from the prolonged and neglected indwelling vesical catheter; the associated stone burden vis-a-vis the duration of neglected indwelling bladder catheter can be seen at 3 months (B), 6 months (C) and 10 months (D). (A) Cystolithotomy image showing the stone (white arrow) and the ruptured balloon (Black arrow) as evidence of failed attempt at removal of retained urethral catheter from a secondary referring facility. (B) Suprapubic cystostomy catheter removed after local lidocaine infiltration adjacent to the cystostomy site. Panel (C) is the catheter with associated stone and fragments of the patient in (A). Panels (C) and (D) are retained urethral catheters with vesical calculi cut distally to enable removal through cystolithotomy wound. The stones volume in (C) and (D) are (4 cm × 3 cm) and (8 cm × 6 cm), respectively.
The second case was a 58-year-old farmer and known patient of our facility who presented in 2021 with acute urine retention following blockage of an indwelling urethral catheter inserted 6 months prior to presentation. The attempt at removal from the secondary referral facility was unsuccessful. He had had substitution Urethroplasty in our facility 6 years before the urine retention for which urethral catheterization was successful and diagnosed to be having bladder outlet obstruction due to benign prostatic enlargement. He was counseled and given medical therapy and for subsequent urethral catheter removal but defaulted to follow-up.
The physical examination and vital signs were within normal range. The laboratory investigations were unremarkable. Transabdominal Ultrasound scan showed hyperechoic appearance at the region of the urethral catheter balloon casting posterior acoustic shadowing. He was counseled and had cystolithotomy, a specimen as shown in Fig. 1C.
The third case was a 65-year-old farmer who was referred from a secondary health centre to our facility in 2015 with fever, painful suprapubic swelling despite in situ suprapubic catheter though not draining for 2 weeks prior to presentation. The SPC was done because of failed urethral catheterization 10 months earlier when he presented at the same facility with acute urine retention secondary to benign prostatic enlargement. He did not return to the facility for follow-up or change of the catheter until the onset of present complaints.
Physical examination revealed an acutely ill-looking elderly man, in painful and respiratory distress, pale, dehydrated and febrile (temperature 39.1°C). The respiratory rate was 26 cycles per minute and tachycardic (pulse rate 110 beats per min) with a blood pressure of 100/60 mmHg. The digital rectal examination was suspicious of prostate cancer. Prostate specific antigen was 14.6 ng/ml. There was leukocytosis with neutrophilia. The Transabdominal ultrasound scan showed hyperechoic structure at the region of the suprapubic catheter balloon casting posterior acoustic shadowing and urine containing multiple echogenic materials.
He was diagnosed of urosepsis secondary to vesical calculus from prolonged and neglected indwelling suprapubic vesical catheter. He was resuscitated with intravenous fluids, transnasal oxygen, intravenous antibiotics and blood transfusion. He was counseled and had cystolithotomy and suprapubic cystostomy, specimen as shown in Fig. 1D. He was later confirmed of prostate adenocarcinoma and managed accordingly.
DISCUSSION
Vesical calculus is a common bladder pathology. In our environment, upper urinary tract calculi involving the kidneys and ureters appear to be commoner accounting for 10.7% of newly diagnosed urological cases annually and coming third after benign prostatic enlargement and bladder tumor [2]. Notwithstanding, it is interesting and noteworthy to underscore rare and avoidable causes of vesical calculus which this paper seeks to do. Over 7 years from 2015 to 2022, three patients were seen in our clinical practice with vesical calculus due to prolonged and neglected indwelling catheters. All the stones were diagnosed using combined clinical evaluation and transabdominal ultrasound scanning, while cystolithotomy was the primary treatment (Fig. 1A). One patient had the suprapubic catheter removed after local lidocaine infiltration adjacent to the cystostomy (Fig. 1B). Two patients had cystolithotomy (Fig. 1C and D).
The causes of vesical calculus can be from various conditions that can lead to infravesical obstruction ranging from posterior urethral valves [5] seen in young age to urethral stricture [6], benign prostatic hyperplasia [7], prostate cancer [8] and bladder neck stenosis [9] among other things seen in adults. The obstruction results in urinary stasis which facilitates crystallization of salts constituents of the urine in the bladder. The stasis also promotes multiplication of microorganisms leading to infection which promote stone formation in the bladder by urease splitting organisms [10].
Foreign bodies are another predisposing factor to vesical calculus formation. Their introduction can occur in individual with psychoaffective disorders or migrate into the bladder from organs contiguous to it such as uterus or placed in the bladder for the purpose of therapy and for erotic purposes [11–15]. Their presence in the bladder especially when prolonged can cause urinary tract infection. They can serve as nidus for stone propagation [12, 15]. The index cases vesical calculus were related to prolonged and infected indwelling vesical catheter [3]. This aetiopathological phenomenon of vesical calculus formation is well known but rare. This is also an avoidable cause of bladder calculus in most parts of the world where access to health care services is not from out-of-pocket expenses. Therefore, the government needs to find a more enduring replacement of this form of health care delivery system to prevent future occurrence.
The diagnosis of patients with prolonged and neglected indwelling vesical calculus requires the combination of clinical evaluation and imaging investigations. All the index patients gave a history of indwelling vesical catheter lasting longer than a month. This history can heighten the index of suspicion of difficult change or removal of the catheter. The imaging investigations that can further confirm the suspicion of vesical calculus include transabdominal ultrasound scan, plain abdominal radiography and computerized tumor graphic scan [16–18]. The choice of these imaging investigations should be guided by a number of reasons among which are availability, accessibility, affordability and consideration for radiation exposure [18].
In a well-trained hand, transabdominal ultrasound scan meets most of these requirements. Since it is readily available, cheap, devoid of radiation exposure and accessible in most of the facilities. All the index cases had transabdominal ultrasound scans which suffice in the index cases for guiding the decision for definitive intervention. It has a short learning curve, and typical diagnostic findings of vesical calculus are the appearance of echogenic structure casting posterior acoustic shadowing associated with the vesical portion of the indwelling catheter. It can also suggest the presence of obvious vesical mass. This may often suffice and guide the decision for treatment. Its limitation includes decreased sensitivity, specificity and accuracy of detecting specific stones as the stone size gets smaller [19].
Other investigations are equally useful. However, a plain abdominal radiograph can diagnose radiopaque vesical calculus but will miss radiolucent stones and vesical mass. The computerized tomographic scan especially the non-contrast film is the gold standard imaging modality for investigating urolithiasis. It can diagnose both smaller vesical calculus and mass but is expensive, may not be readily available and associated with significant radiation exposure [20].
Once a significant stone burden is established around an indwelling catheter, non-invasive removal using chemolysis presents an enormous task. The various notable methods of vesical calculus treatment include extracorporeal shock waves lithotripsy, transurethral cystolithotripsy, percutaneous cystolithotripsy, laparoscopic approach, combined percutaneous approach and transurethral cystolithotripsy, transurethral cystolitholapaxy and cystolithotomy depending on the available facilities [4, 21]. Cystolithotomy was the primary modality of treatment use in the majority of the cases reported here.
CONCLUSION
Vesical calculus arising from avoidable aetiology such as prolonged and neglected indwelling catheters is rare but still possible. Cystolithotomy may be necessary and rewarding. Therefore, these cases draw the attention of attending healthcare workers to proper patient education, guidance and counseling during patients’ visits to health facilities.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
No funding was obtained for this study.
ETHICAL APPROVAL
The clinical picture meets ethical guidelines and adheres to the local legal requirements.
CONSENT
Informed consent was obtained from the patient.
GUARANTOR
K.A.

{kind=link}