





Abstract
Foreign body ingestion is a common condition in daily practice; fortunately, most cases do not require endoscopic or surgical treatment, as most foreign bodies pass through the intestine without injuring it. Although mainly seen in children, adults can also be affected, especially in accidental situations and suicide attempts. Therefore, the clinical history and the environment in which the event occurred are essential for a rapid diagnosis. This can be even more challenging as most adult patients are rarely aware of ingestion. Therefore, a high index of suspicion is necessary. Therapy will depend on the foreign body’s size, shape and material; treatment should not be delayed if complications are detected. We present a case of a 34-year-old man who accidentally swallowed the mold of his teeth while undergoing a dental procedure. Subsequently, he presented with an intestinal obstruction that required surgery. Fortunately, he made a full recovery.
INTRODUCTION
Treating patients with ingested foreign bodies is common in clinical practice [1]. However, a difference is made between accidental ingestion of a foreign body and intentional ingestion [1, 2]. In adults, the most commonly swallowed adults are fish bones, bones and dentures. Most foreign bodies will pass (80%) without complications; nonetheless, despite the usually benign course, it can be associated with severe complications that may need endoscopic or surgical interventions [1].
We present the case of a healthy young man who, after accidentally swallowing his dental mold during a dental impression, developed an intestinal obstruction that required surgery. He underwent full recovery.
CASE REPORT
An otherwise healthy 34-year-old man was admitted to the emergency department. Eighteen hours before his admission, he accidentally swallowed the mold while having a dental impression taken during the dentist’s consultation. He was advised to go to the emergency department immediately, but as he felt fine and was very fearful, he decided not to go. Six hours passed after the event, and he did not feel any pain or discomfort; however, after this time, he began to feel a slight abdominal pain in the epigastrium; 2 h went by, and the pain increased in intensity until it became unbearable, then nausea appeared, followed by severe episodes of bilious vomiting and the impossibility to expel gas or stool.
On clinical examination, a dehydrated patient with tachycardia was encountered with significant abdominal distention, diminished bowel sounds, and severe abdominal pain on palpation with tenderness. Complementary exams revealed metabolic acidosis (pH < 7.2) and a serum lactate level over six mmol/L. After exhaustive reanimation, imaging tests were needed. Unfortunately, X-rays and computed tomography (CT) were not available at that time; therefore, an abdominal ultrasound was done, but it was not helpful as gas was present. After adequate resuscitation, the patient’s condition improved, and we were able to transfer the patient for the much-needed imaging tests.
The abdominal CT revealed severe distention of small bowel loops, compatible with intestinal obstruction, and a hyperdense 4 x 3 cm foreign body in the lumen of the jejunum. Surgical consultation was needed, and with these findings, surgery was planned (Fig. 1A and 1B).
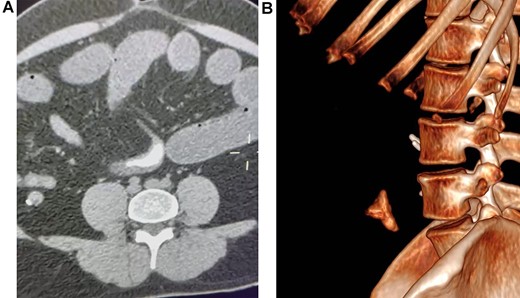
(A) Abdominal CT, revealing a foreign body in the lumen of the bowel. (B) CT reconstruction of the foreign body.
On laparoscopy, the full extent of the bowel was dilated, and the foreign body was discovered 1.80 m proximal to the ileocecal valve; then, the bowel was grasped and extracted through the umbilical port. After placing a skin protector, a 3-cm longitudinal incision on the antimesenteric side of the bowel was done, the foreign object was extracted, and the enterotomy was closed in a transverse fashion in two layers. No perforation, necrosis, or free fluid was found, and the remainder of the procedure was completed without complications (Fig. 2A and 2B).
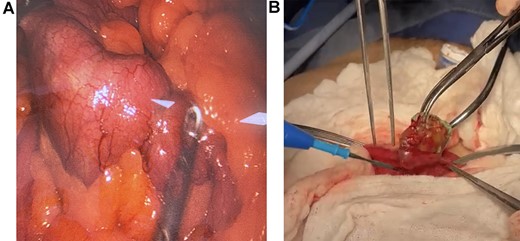
(A) Laparoscopy, the foreign body is found in the bowel. (B) Extraction of the foreign body through enterotomy.
A 4 x 4.5 cm alginate dental mold shaped like a U was retrieved. Bowel obstruction due to accidental body ingestion was the final diagnosis (Fig. 3).

Alginate dental mold.
The patient was closely monitored during his hospitalization. Finally, after tolerating a complete diet, he was discharged without complications. On follow-up, he is doing well.
DISCUSSION
Accidental ingestion of foreign bodies is a common occurrence in everyday life [1]. Although it is a condition that usually occurs in young patients, it can also occur in adults, as an accident (alcoholism, dental problems, etc.) or with secondary gain. (Incarceration, suicide) [1, 2].
A wide variety of ingested objects have been reported, from coins, pins, nails, toothbrushes and teaspoons to dental bridges [2, 3]. Ingested foreign bodies usually do not cause problems; however, they can cause intestinal obstruction if they become trapped; this usually occurs in the ileocecal region, appendix, sigmoid colon and rectum [1, 2]. However, any area can be affected, especially in patients with bowel disorders such as adhesions or inflammatory bowel disease [1, 4].
Diagnosis of foreign object ingestion can be problematic, especially if the patient does not recall swallowing the object [2]. In most patients, clinical signs are usually mild and can even be lacking as long as no occlusion or perforation develops [2, 3]. Symptoms can vary from difficulty in swallowing to chest discomfort, abdominal pain or vomiting [2]. Without a clear history, diagnosis becomes difficult; therefore, a very high clinical suspicion is needed [3, 5]. Metallic objects can be easily seen on a plain X-ray, and more advanced studies such as endoscopy or CT can help us locate the foreign object within the gastrointestinal tract [6].
In our case, the patient had a clear history that allowed a more straightforward diagnosis; however, surgery was required since he had symptoms of bowel obstruction.
The intrinsic characteristic of the ingested object will significantly impact the patient’s outcome [2, 4, 7]. For example, sharper objects such as chicken bones and toothpicks carry a greater risk of intestinal perforation, peritonitis and sepsis; this is because the continuous pressure of the foreign body into the bowel wall will cause ischemia necrosis and ultimately destruction of the underlying mucosa and muscle [5, 8]. Objects larger than 5 cm should also be removed because they will not be able to pass the pylorus or ileocecal valve, causing obstruction [1, 5]. In our case, the size of the foreign object obstructed the bowel and caused this complication.
Treatment will depend on the time since ingestion, the size and characteristics of the foreign object; for example, if the foreign body is in the cricopharyngeal sphincter, esophagus or stomach, endoscopic removal is recommended [6, 8]. This can ensure a shorter hospital stay and no complications [5, 9]. Nonetheless, if endoscopic measures fail, observation is recommended as the initial plan if the foreign body passes the duodenum because most objects will pass without complications [1, 10]. A waiting period of 3 days to 2 months before surgery has been proposed because the risk associated with a laparotomy may outweigh any potential benefits of removing a non-sharp foreign body [2, 3].
In our case, as the patient came late to the emergency department due to fear and lack of confidence, endoscopic treatment was not possible; furthermore, surgery was necessary as a foreign object was found in the intestine and caused an intestinal obstruction. One particular thing to mention is that if the foreign body is a battery, the chemical injury that these objects could cause to the intestinal mucosa can lead to a higher rate of complications, so a faster removal is recommended [11–13].
Each case must be individualized when approaching an ingested foreign body, and treatment will depend on the object’s location and potential for perforation. If symptoms appear, more aggressive treatment is necessary to remove the foreign entity to prevent perforation and peritonitis.
Complications
Prevention of ingestion seems to be the best treatment approach to prevent ingestion of foreign bodies. Treatment will be determined by the type of foreign body (size, length, composition), symptoms and clinical findings. Uniquely, this case again proves that time is of the essence in medicine and that prompt treatment could avoid serious complications.
FUNDING
None.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}