





Abstract
A 66-year-old female without prior history of abdominal surgery visited the emergency department with a complain of sudden intensive lower abdominal pain. Closed loop bowel obstruction was discovered on contrast-enhanced computed tomography, leading to a laparoscopic examination of 5 h after the onset. During laparoscopy, 100 cm of distal jejunum with borderline viability was found incarcerated in a gap of the greater omentum. A 3-cm small incision was made at the umbilical trocar site to observe the bowel after it was released laparoscopically. When viewed under the shadowless lamp, the affected bowel appeared reddish, with peristalsis and a palpated mesentery artery. The surgical team determined no need for resection. The postoperative recovery went smoothly without any complications. Laparoscopic surgery for transomental hernias can be performed safely even in patients with borderline bowel viability, and observing bowel extra-peritoneally with a small incision could be helpful for laparoscopic surgery for internal hernias with borderline viability.
INTRODUCTION
Transomental hernia is a type of internal hernias of the bowel and is a rare cause of small bowel obstruction (SBO) [1]. The prevalence of internal hernias in SBO is low at |$\sim$|6%, but transomental hernias among internal hernias are even rarer, accounting for 1–4% of internal hernias [1, 2]. The majority of transomental hernias in adults are iatrogenic (post-surgical) or post-traumatic. In rare cases, senile atrophy of the omentum may lead to spontaneous herniation of the small bowel loop in the virgin abdomen [1, 3]. On the other hand, since transomental hernia can cause strangulation or incarceration even in a virgin abdomen, if the diagnosis is delayed, it can lead to bowel necrosis, which could be fatal and requires urgent surgical intervention [1]. Recent improvements in surgical techniques have allowed laparoscopic surgeries for transomental hernias to be carried out safely without evidence of necrosis or perforation [3–5]. However, there is not enough information on whether the laparoscopic technique can be used safely for strangulated hernias with severe bowel viability, since no clear criteria are available to evaluate the viability of a strangulated bowel, particularly in laparoscopic surgery.
In this report, we have presented a case of transomental hernia with borderline viability of the strangulated bowel, in which laparoscopic surgery was performed with a small laparotomy to evaluate the bowel and avoid resection.
CASE PRESENTATION
A 66-year-old female without any history of abdominal surgery or medical problems experienced a sudden intensive lower abdominal pain at 4 a.m. while sleeping. Her family contacted the emergency medical system, and she was transported to our emergency department (ED). Her vital signs at the ED showed tachypnea, but no signs of fever. On physical examination, her abdomen was soft, but there was a rebound tenderness in her right lower abdomen. No abnormalities were found in the laboratory tests, except for an elevated creatinine kinase of 250 IU/L (reference range: 41–153 IU/DL). Contrast-enhanced computed tomography revealed closed loop bowel obstruction in the right lower abdomen. (Fig. 1) Since the patient had a virgin abdomen, a diagnosis of internal hernia secondary to physiological intra-abdominal adhesions was made and laparoscopic examination was initiated 5 h after the onset of abdominal pain.
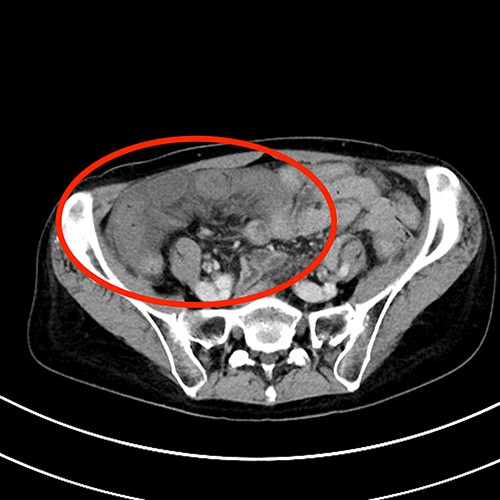
Contrast-enhanced abdominal computed tomography findings. Small bowel loops with caliber change and edematous mesentery are in the right lower abdomen.
Laparoscopy revealed that 100 cm of distal jejunum was incarcerated in a gap of the greater omentum, which hangs down from the transverse colon and is physiologically adherent to the ascending colon. The strangulated bowel appeared black/purple in colour. Using an ultrasonic instrument (SonoSurg, Olympus©️, Japan), the adhered greater omentum was cut from the gap toward the proximal ascending colon, and incarceration was released. It was difficult to determine the viability of the bowel from the colour only under the laparoscope, so a 3-cm small incision was made at the umbilical trocar site, which allowed visualization and palpation of the entire length of the involved bowel and mesentery. The affected bowel appeared reddish when viewed under the shadowless lamp (Fig. 2A and B). Furthermore, the surgical team noticed peristalsis and palpated the mesentery artery, which led them to conclude no resection was required. To determine the need of the second look surgery, a drainage tube was placed in the abdominal cavity. The postoperative recovery went smoothly without any complication, and the drainage tube was removed on Day 5. The patient was discharged from the hospital on Day 14.
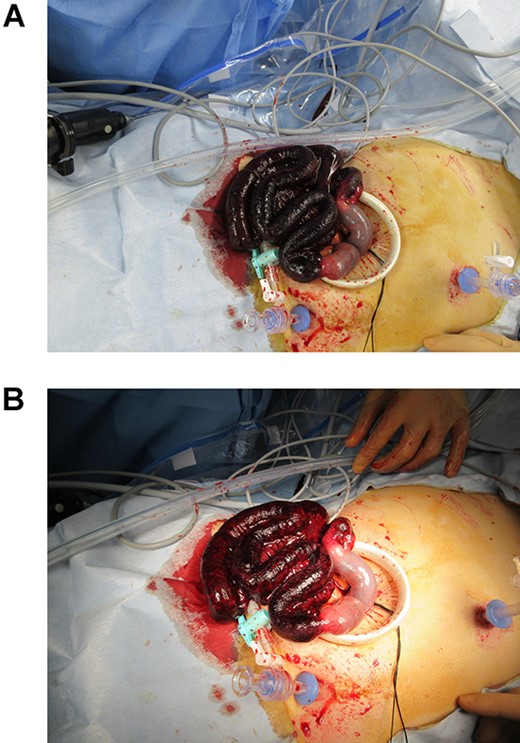
Intraoperative photographs of the bowel after small laparotomy. (A) Without a shadowless lamp, the involved bowel was black/purple in colour. (B) Under a shadowless lamp, the affected bowel appeared reddish.
DISCUSSION
In this case, we demonstrated a patient with strangulated transomental hernia whose bowel viability was difficult to determine. Successful laparoscopic surgery was performed with the aid of a small incision and shadowless light, leading to the successful preservation of the affected bowel. This case highlights two main points (i) laparoscopic surgery for transomental hernia can be performed safely even in patients with borderline viability of the intestine; (ii) observing bowel extra peritoneally with a small incision and a shadowless light could be a reasonable procedure to determine the viability of the intestinal tract while undergoing laparoscopic surgery for an internal hernia.
Laparoscopic surgery can be performed safely in the cases of internal hernias, such as transomental hernias, in the virgin abdomen, particularly with borderline to severe bowel viability. According to the past literatures, most transomental hernias surgeries have been performed through laparotomy [3]. To the best of our knowledge, among the few reports of laparoscopic surgery, most procedures were carried out only by laparoscopic technique to release the incarceration [3, 4, 6, 7]. As in this case, when it is difficult to assess the viability of the bowel, open laparotomy was chosen over laparoscopic surgery for transomental hernia because laparoscopy alone was not considered sufficient to determine the bowel viability [4]. Certainly, the indication of laparoscopic surgery for the transomental hernias should be carefully considered to prevent the risk associated with inadequate observation of the involved bowel by laparoscopy. However, this case suggests that laparoscopic surgery can be performed safely even in cases of internal hernias with borderline or severe bowel viability.
During a laparoscopic surgery for the SBO with strangulated bowel, it may be beneficial to remove the involved tract extra peritoneally using a small laparotomy to confirm the bowel viability. In previous studies, several types of objective measures, such as pulse oximetry, spectrophotometry and fluorescence imaging with indocyanine green, have been proposed to confirm the viability of the intestinal tract intraoperatively [8]. On the other hand, as of today, no gold standard guideline is established for evaluating bowel viability; thus, during a surgical procedure, surgeons ultimately have to determine bowel viability based on subjective indicators and their own experience. By adding a small laparotomy to laparoscopic surgery, the surgeon gains a better understanding of the intestinal tract by physically touching and seeing it, though, of course, that does not always suffice to evaluate it. Moreover, the ability to observe the strangulated bowel under a shadowless light could be highly useful, as is in this case. For these reasons, surgeons should not hesitate to add a small laparotomy to laparoscopic procedures.
AUTHORSHIP STATEMENT
Sawano T, Kurokawa T, Furuya M and Kanzaki N managed the patient. Sawano T wrote the manuscript. Other authors made substantial contributions to the designing of the study and critical revision of the manuscript.
ACKNOWLEDGEMENT
The authors express their sincere gratitude to the clinical radiologists of Jyoban Hospital of Tokiwa Foundation for their technical cooperation.
CONFLICT OF INTEREST STATEMENT
Ozaki A receives personal fees from MNES Inc., outside the submitted work. The other authors declare no competing interests.
FUNDING
None.
PATIENT CONSENT
A written consent has been obtained before submission and be made available to the publisher if requested.

{kind=link}
{kind=link}