





Abstract
Cardiac myxoma is a benign primary cardiac tumor. Herein, we report a case of mitral regurgitation due to annular dilatation caused by giant left atrial myxoma. The transthoracic echocardiogram performed in a 65-year-old man who suffered from worsening exertional dyspnea detected a large mass of 81 × 31 mm in the left atrium, causing functional severe mitral stenosis. Radical mass resection was performed. After removal of the aortic clamp, an intraoperative transesophageal echocardiogram revealed moderate mitral regurgitation due to annulus dilatation. Mitral annuloplasty was performed, and mitral regurgitation was controlled. The mass was diagnosed as myxoma histologically. A large myxoma that affects mitral annulus dilatation is rarely reported. Mitral regurgitation may be masked by the presence of a large myxoma. Therefore, it should be carefully evaluated after resection, and mitral annuloplasty should be considered in the presence of significant mitral regurgitation due to mechanical annulus dilatation caused by myxoma.
INTRODUCTION
Myxoma is a benign primary cardiac tumor mainly occurring in the left atrial (LA) cavity and often not involved in the mitral valve. However, we report a case of giant LA myxoma indirectly affecting mitral annulus dilatation requiring annuloplasty.
CASE REPORT
A 65-year-old man on hypertension and hyperlipidemia medications had decreased systemic blood pressure 2 months before presentation; thus, his antihypertensive medication was discontinued by his home doctor. He felt fatigue and loss of appetite and body weight loss of 5 kg for 6 months. Back pain and cough occurred 1 month before presentation. He went to a general hospital with complaints of continuous exertional dyspnea 2 weeks before presentation.
His vital sign was stable. Chest auscultation revealed an increased apical first heart sound. His chest X-ray detected cardiac enlargement (cardiothoracic ratio, 57%) and increased pulmonary markings. An electrocardiogram showed sinus tachycardia and a negative T wave in leads V1–V4. There were no episodes suspected paroxysmal atrial fibrillation. A transthoracic echocardiogram revealed a giant mass of 81 × 31 mm attached to the interatrial septum in the left atrium (Fig. 1A). The mass was floating and prolapsed into the left ventricle through the mitral valve orifice during diastole (Fig. 1B). Effective mitral orifice and mean pressure gradient via the mitral valve were |$\sim$|0.73 cm2 and 9 mmHg, respectively, and the mass affected for hemodynamics was equivalent to severe mitral stenosis. Mitral annulus was dilatated to 30 × 35 mm, and mild mitral valve regurgitation was observed. Enlargement of left atrium was 43 mm in the anteroposterior diameter. Right atrial and ventricular dilatation, moderate functional tricuspid valve regurgitation and severe pulmonary hypertension with the right ventricular systolic pressure of |$\sim$|88 mmHg were also observed. Biochemical tests showed that a high brain natriuretic peptide value of 661 ng/ml and tumor markers of carcinoembryonic antigen(CEA), CA19–9, interleukin-2 receptor were within the normal limits. He was diagnosed with congestive heart failure of NYHA III due to a giant mass. No clinical findings of cerebral infraction were observed. He was then transported to our hospital. Urgent surgical mass resection and tricuspid annuloplasty were planned.
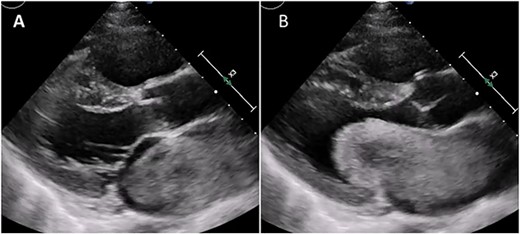
Transthoracic echocardiogram during systole (A) and diastole (B). Giant LA myxoma was prolapsing to the mitral valve orifice.
Median sternotomy was performed, and cardiopulmonary bypass was established via aortic and bicaval cannulation. Under cardiac arrest with antegrade cardioplegia perfusion, the LA was examined via the transseptal approach. The LA cavity was filled with the mass that the stalk was attached to the septal wall at the LA side, and the mass was too big and resected in pieces (Fig. 2). The mitral valve leaflet was intact, and the atrial septum was closed. Dilatated tricuspid annulus was fixed using a flexible band (Tailor Flexible band 29 mm, Abbott). After unclamping of the ascending aorta, a transesophageal echocardiogram points out moderate mitral regurgitation due to mitral annulus dilatation (Fig. 3). Cardiac arrest was performed again, and mitral annuloplasty was performed with a semi-rigid ring (Carpentier-Edwards Physio Ring II 26 mm, Edwards) via left atriotomy. His heart sinus rhythm returned to normal with successful weaning from cardiopulmonary bypass. After the transesophageal echocardiogram procedure, no evidence of the mass and residual mitral regurgitation was confirmed (Fig. 4).
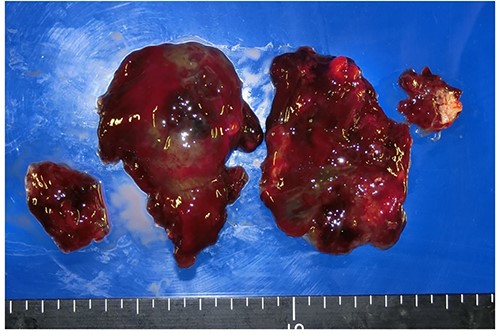
Resected specimen of myxoma.
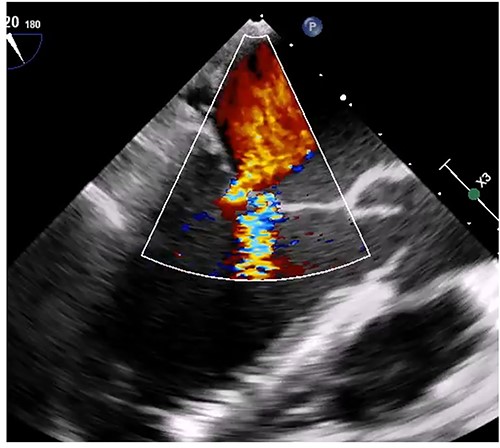
Intraoperative transesophageal echocardiogram after the myxoma resection. Moderate mitral regurgitation with annulus dilatation was detected.
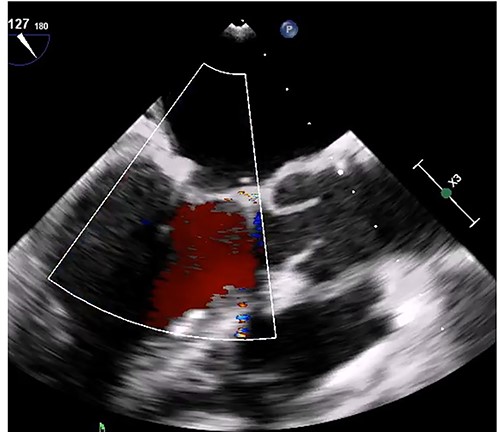
Transesophageal echocardiogram after mitral annuloplasty. There was no residual mitral regurgitation.
No signs of a cerebral event or surgical site infection were observed, and his clinical course was good. The resected specimen was a dark-red and jelly-like fashion. In histological examination, the tumor was confirmed to be comprised of a spindle or globular myxoma cells with abundant lightly eosinophilic to basophilic cytoplasm consistent with myxoma.
DISCUSSION
Primary cardiac tumor rarely occurs, with the incidence of 0.0017–0.33% in autopsy [1]. Myxoma is a benign primary cardiac tumor, comprising |$\sim$|50% of all benign cardiac tumors in adults. Generally, most myxomas occur solitary and are located in the left atrium (75%) and the right atrium (10–20%) [2, 3]. Myxomas are often detected accidentally because of their asymptomatic nature. Although this patient suffered from congestive heart failure due to severe mitral stenosis, immediate surgical treatment tends to be performed for giant or fragile myxoma that may cause circulation collapse or systemic embolization.
Radical resection is sufficiently effective for typical LA myxoma pedicled atrium without valve dysfunction, and the majority of myxoma have a low recurrence rate [3, 4]. Additional procedures sometimes are required in tumors that reached the valve leaflet or are accompanied by chordal dysfunction [5]. Mitral annulus dilatation due to the tumor is uncommon [6] and considered to be caused functionally by LA dilatation due to mitral stenosis or directly mechanical compression from the large myxoma. Mechanical annulus dilatation was considered in our patient because of no LA dilatation and relatively short-valve leaflet in respect to the annulus. This type of mitral dilatation might result in postoperative remodeling. However, Matsushita reported the case of a patient with deteriorated mitral regurgitation requiring surgical repair 1 year postoperatively [7]. Giant LA myxoma might mask preoperative mitral regurgitation due to annulus dilatation, and thus intraoperative assessment by transesophageal echocardiogram is important. Mitral annuloplasty should be considered in the presence of significant mitral regurgitation due to mechanical annulus dilatation caused by myxoma.
CONFLICT OF INTEREST STATEMENT
All authors have no conflicts of interest.

{kind=link}
{kind=link}
{kind=link}
{kind=link}