





Abstract
Cystic lymphangioma is a benign congenital disease that is more seen in head and neck regions. We report a case of a 54-year-old man with a growing supraclavicular mass. The ultrasonography and magnetic resonance imaging suggested a cystic lymphangioma. The mass was surgically totally removed without any recurrence. Histology examination confirmed the diagnosis. Cystic lymphangioma in adults is a rare entity and the literature on the subject is poor with no global recommendations.
INTRODUCTION
Cystic lymphangioma is a benign congenital disease characterized by a malformation of lymphatics structures with aberrant proliferation of lymphatic vessels resulting in a large cystic formation [1]. It can affect any anatomic site, but it is more seen in head and neck, followed by clavicle and axillary regions. It is supposed that it is due many lymphatics being encountered in these areas. The affection is diagnosed usually in the childhood (0–2 years) (80%–90%) with an incidence of 1.2–2.8 per 100 000 children [2]. An adult’s presentation is rare de facto. The literature on the subject is poor with no global recommendations. With this case report we want to contribute to the body of literature on the subject that can lead to future global recommendation of management.
CASE PRESENTATION
A 54-year-old man presented in clinic for a supraclavicular mass. The patient swam a lot and the mass had been painful for a few weeks. He suffered from hypertension controlled by medications. He had amygdalectomy during childhood and knee-arthroscopy in 2013. Formerly an ultrasonography (US) was performed and revealed a single cystic mass in the right supraclavicular superior and lateral to the brachial plexus and the subclavian vessels, measured at 35 × 17 mm, thin-walled, without associated nodular or tissue formation and without abnormal vascularization. Fine needle aspiration (FNA) was carried out using US and revealed small lymphocyte-like cells mixed with lymphedema-like material. The cyst reccured rapidly after the puncture. Clinically the mass was renitent, moveable and nonadherent. Magnetic resonance imaging (MRI) showed a right supraclavicular cystic formation antero-superior to the subclavian vessels, measured at 43 × 40 × 27 mm, thin-walled, no fleshy component nor associated nodular formation, without tissue enhancement after injection of gadolinium (Fig. 1). A diagnosis of a cystic lymphangioma was retained. A supraclavicular incision was performed under general anesthesia. The cyst was dissected gradually and we ligated and clipped the base of the cyst. The cyst was removed completely (Fig. 2). After hemostasis, a surgical drain was set. The skin was sutured in two layers. There was no postoperative complication. The drain was removed the day after surgery and we discharged the patient at home. The histopathological exams reveal a cystic wall very thinned, bordered by endothelium without any atypical shape and lymphoid tissue without any atypia, confirming the diagnosis of a cystic lymphangioma. No relapse occurred during the follow-up of >3 years.
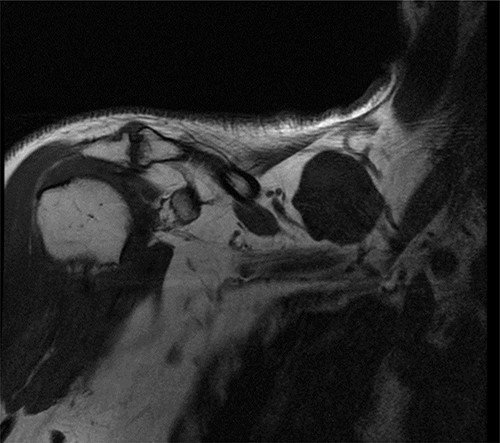
T1-weighted MRI sequence showing a supraclavicular cyst.
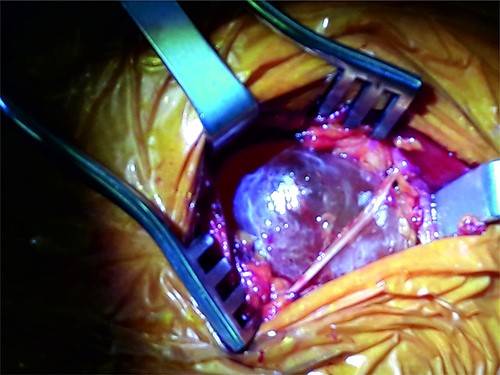
Cyst removal.
DISCUSSION
Cystic lymphangioma is a benign malformation of lymphatics structures. It is more seen in the head and neck area and the clavicular and axillary regions, but any anatomic site can be affected. The supposed etiopathology in adult presentation are lymphatic obstruction with lymph fluid retention caused by trauma, infection or neoplasm but it is still controversial [3, 4]. The differential diagnosis of a cervical mass is various with the most important as a branchial cyst, thyroglossal cyst, adenopathy accounting for >90%. More specifically, a supraclavicular mass could be a lymphoma, an adenopathy, a carcinoma, mycobacterial or fungal infection but also can be the first manifestation of an unknown abdominal or thoracic carcinoma. Clinical presentation depends on the location, size and rate of growth. By growing, the tumor tends to compress structure like trachea, esophagus and can cause dyspnea and dysphagia [5]. In the clavicular or axillary regions, it can also compress great vessels and could lead to a superior cave syndrome with Claude-Bernard-Horner sign, some plexus brachial lesions, … Because of the rarity and the benignancy of this entity, it is important to exclude the diagnosis behind the type of presentation. The investigations are usually made by with computed tomography (CT), MRI or US. US is the first exam to ask to investigate a cervical mass. It is heap, nonirradiant and noninvasive. The use of FNA is controversial. Some authors recommend it, but other authors defend that FNA is a source of iatrogenous infection and increasing the risk of bleeding or recurrence [6]. The US will show an anechoic cystic cavity with or without multiloculations. On CT, the lesion is a homogeneous cystic mass without enhancement after intravenous contrast injection. The MRI characteristics of these type of tumors are a low to intermediate intensity on T1-weighted images, hyperintensity on t2-weighted images and no enhancement after gadolinium injection [7]. The definitive diagnosis is made by histopathology examination. The surgery stays the gold standard of treatment [8–10]. Complete surgical removal is an important modality. The recurrence rate if not completely removed after surgery is about 10%–15% [9]. Cystic lymphangioma tends to infiltrate neurovascular structure and muscles especially in children [8]. Theses tumors are well-circumscribed in adults. Thereby complete surgical excision is relatively easier compared to pediatric population. Some of these tumors are spreading along vital structure and the removal in totality is unavailable by surgery. Alternating therapies are available like sclerosis by chemical drugs, radiotherapy or laser therapy. Sclerosis or laser therapy are usually preferred in children [10, 11]. Radiotherapy was successfully used in the past but because of the potential risk in children, its use is limited [11]. In adults, these therapies are used to treat a relapse or in adjuvant therapy after surgery.
CONCLUSION
As the incidence of cystic lymphangioma in adult is rare, the nature and reporting of their management is limited. This case report contributes to the body of literature which serves for future global recommendation of the optimal management of this perinatal condition in adults.

{kind=link}
{kind=link}