





Abstract
Infrared thermography is a useful adjunct for the clinical monitoring of infantile hemangioma (IH) activity with or without treatment. There is a dearth or reporting on the ideal tissue for standardizing temperature readings from IH. This case illustrates the use of mean medial canthal temperatures and the differential hemangioma temperatures for monitoring of facial IH.
INTRODUCTION
Infantile hemangiomas (IHs) are the commonest infantile neoplasm with an incidence of 1–3% in Caucasians [1]. A lower incidence is reported in Blacks [2]. They are benign vascular tumors appearing shortly after birth as a herald reddish patch. The diagnosis of IH is clinical in 90% of cases [1, 2]. The natural history of IH is characterized by rapid proliferation up to 6–12 months, a plateau phase and subsequent involution [1–3]. This natural history lends itself to conservative management in most cases of IH. Treatment is necessary where the hemangiomas are functionally debilitating such as affecting the visual field in periorbital hemangiomas or causing respiratory obstruction when located anywhere along the respiratory tract [1, 4, 5]. Hemorrhage, ulceration or serious disfigurement are other indications for treatment [1, 2]. Adjuncts to aid diagnosis and management include color doppler ultrasonography, magnetic resonance imaging (MRI), computed tomography (CT) scan and infrared (IR) thermography [2, 6]. IR thermography is useful in the assessment and monitoring of IH [6, 7]. Studies utilizing IR thermography have used the visual analog scale or subjective clinician and patient reports to validate its use. This case presentation illustrates the use of the mean medial canthal and differential hemangioma temperatures (DHTs) for IR thermographic monitoring of facial IH.
CASE REPORT
A 7-month-old child was brought to our clinic by her mother with complaints of a reddish disfiguring large lesion on her lower lip. There had been a reddish hue at birth. This was followed by a rapid increase in size over the subsequent weeks to become disfiguring and prevented the child from closing her mouth (Fig. 1a). There were no lesions anywhere else. Examination revealed a hyperemic disfiguring lesion on the lower lip, which was soft, doughy with differential warmth. It was compressible but not pulsatile. A diagnosis of IH was made. With the use of a Flir One Camera, a thermographic temperature reading of the lesion, as well as that of the medial canthal vessels, was taken on the day of presentation (Fig. 2a). She was commenced on oral propranolol at 1 ml/kg/day after ensuring normal electrocardiogram and blood profile. Thermographic temperature readings were taken at every subsequent visit (Fig. 2a, Table 1). A steep drop in the DHT was seen after the commencement of propranolol therapy, pointing to its efficacy (Fig. 3). On her third visit after the commencement of oral propranolol, there was an increase in the DHT (Fig. 3). The mother informed that she had run out of the drug 5 days prior to that visit. The patient was recommenced on oral propranolol. At the follow-up visit 10 months after commencement of propranolol, she was able to close her mouth (Fig. 1b), and the DHT was appreciably low (Fig. 3).
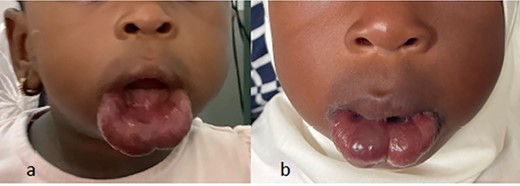
(a and b) Lower lip hemangioma before (a) and after (b) treatment with propranolol.
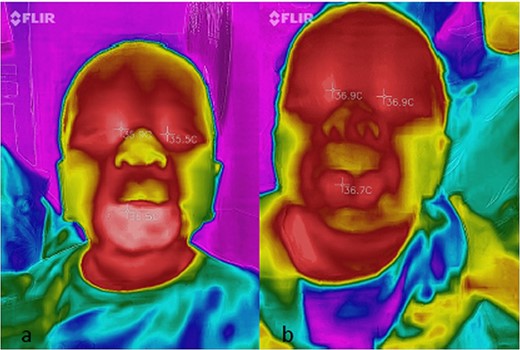
(a and b) Thermographic medial canthal and hemangioma temperature readings before (a) and after (b) commencement of oral propranolol.
Serial IR thermographic readings
| Examinations | Right medial canthal temperature | Left medial canthal temperature | MHT | MMCT | DHT |
|---|---|---|---|---|---|
| 1 | 35.90 | 35.50 | 36.50 | 35.7 | 0.8 |
| 2 | 35.20 | 35.20 | 36.20 | 35.2 | 1 |
| 3 | 33.00 | 32.80 | 33.90 | 32.9 | 1 |
| 4 | 35.00 | 34.60 | 35.00 | 34.8 | 0.2 |
| 5 | 36.90 | 36.90 | 36.70 | 36.9 | −0.2 |
| 6 | 37.00 | 36.80 | 37.50 | 36.9 | 0.6 |
| 7 | 27.60 | 27.40 | 27.70 | 27.5 | 0.2 |
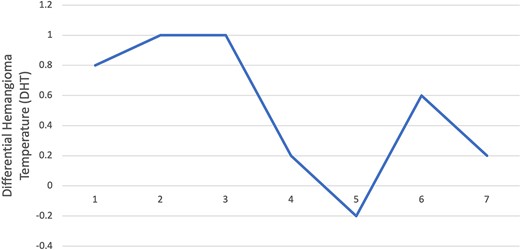
Line graph showing DHTs.
FORMULA FOR CALCULATING MEAN MEDIAL CANTHAL AND DHTS
DISCUSSION
This case presentation demonstrates that the use of DHTs provides more information than absolute hemangioma temperatures (Fig. 4) in the assessment of hemangioma activity or the monitoring of treatment. For facial hemangioma not involving the eyelids, the MMCT can be used as a standard for determination of the DHT.
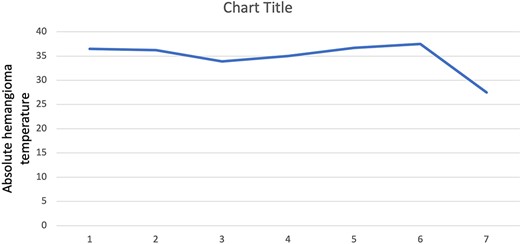
Line graph showing serial absolute hemangioma temperatures.
IR thermography has increased our understanding of the activity of IH, and both static and dynamic IR thermography have been employed in IH activity determination [7–10]. IR thermography is not as expensive as other modalities, such as CT and MRI, in the monitoring of IH. Thermography is a non-contact, non-invasive and useful clinical adjunct for the management of IH. Previous studies have utilized the visual analog scale to determine the effect of propranolol therapy on the activity of IH [6, 8]. Subjective clinical esthetic assessments by either the clinician or patients have also been used [8]. Kalicki et al. suggested that comparison of IH temperatures with an adjacent body part would provide more objective measurements [7]. Given that the hemangioma is a vascular tumor, utilization of a normal vascular activity to standardize the temperature readings has some merit. It obviates any form of subjectivity and can be applied readily as seen in this case. Propranolol has replaced corticosteroid as the first line of treatment for IH where conservative watchful waiting is not feasible [5]. Mechanisms of propranolol activity include vasoconstriction, downregulation of vascular endothelial growth factor and basic fibroblast growth factor as well as upregulation of capillary endothelial cell apoptosis [5, 11]. Although its effects are systemic, the side effects, when given at 1–3 mg/kg, are not as significant as those experienced when using corticosteroids in the management of IH [5]. The rebound phenomenon when use of propranolol is discontinued could be as high as 7% [11]. This was seen in our patient when she discontinued the propranolol. This rebound was also more clearly detected by the DHT than the absolute hemangioma temperature.
CONCLUSION
MMCTs can be used as a standard for objectively comparing infantile facial hemangioma activity or for monitoring the effects of treatment. DHT rather than absolute hemangioma temperature is more informative. These measurements can be used to design subsequent studies on facial hemangioma.
ACKNOWLEDGEMENTS
The author thanks Dr Brett Davis and his team for making available the Flir One camera and Ipad.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
None.

{kind=link}
{kind=link}
{kind=link}
{kind=link}