





Abstract
Congenital aural atresia refers to abnormal embryological development of the external auditory canal. The treatment of this anatomical malformation is only surgical repair. This article reports a case of unilateral congenital aural atresia, the surgical procedure performed and the post-operative findings.
INTRODUCTION
Anatomical malformation of hypoplasia of the external auditory canal is quite rare and is present 1 in 10 000–20 000 births [1]. It can be congenital or acquired after trauma. In case of congenital aural atresia, the etiology is based on normal embryological pattern disruption. Mostly, it is unilateral approximately in 70–90% and it affects the right side because it can be more commonly affected by hypoperfusion than the left, where the heart is located and which generally has a pressure 10 mmHg higher than the right one [2]. In general, aural malformations can be present in a ratio of 1:3800 children. In some of them, bilateral congenital aural atresia may occur when the malformation is not an isolated condition but is in the context of a syndrome, such as CHARGE syndrome, in which newborns are affected by bilateral atresia in up to 60% of cases.
The origins of this anatomic malformation are embryological. It is well known that the aural anatomic structures have a different embryologic origin; the auricle develops from the first and second branchial arches, external canal and tympanic membrane from the first branchial cleft [1, 2]. The closely related development of the external acoustic canal and the middle ear led to the classification of the combined malformation as atresia aural congenital according to the literature [3].Three degrees of severity have been described: first-degree malformations present with mild deformities of the external auditory canal, a normal or hypoplastic tympanic cavity, malformed ossicles and a well-ventilated mastoid. Second-degree deformities are intermediate deformities. These include a blind-ending or absent external auditory pathway, a narrow tympanic cavity, deformities and fixations of the ossicles and decreased pneumatization of the mastoid cells. Third-degree malformations are severe deformities. The external auditory canal is completely absent, the middle ear is hypoplastic and the ossicles are severely deformed. In addition, pneumatization is inhibited.
CASE REPORT
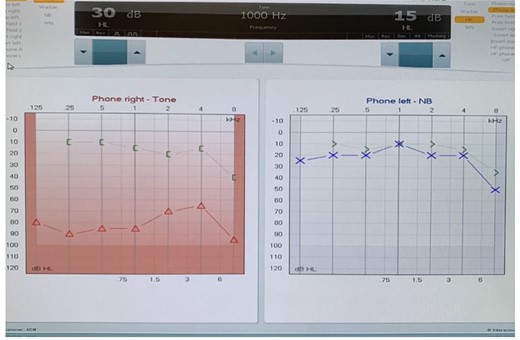
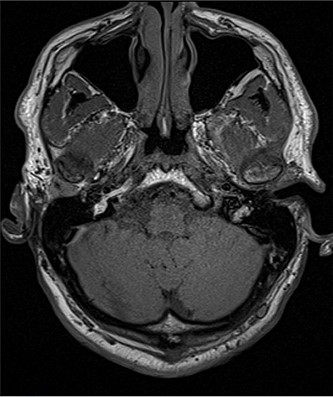
A 56- year old male was presented in the Outpatient Department of Otolaryngology Clinic with main complaint of complete aural atresia of the right ear. The clinical examination revealed that there was no external auditory canal in the right ear (Fig. 1) and hearing loss was altered (Fig. 2). There was no symptomatology in the left ear and the anatomic structures were completely normal. Blood test was normal, and there were no other medical issues from the personal history. The computed tomography (CT) scan and mainly the magnetic resonance imaging (MRI) of the temporal bone revealed no mastoid air cells and no external auditory canal and auricle (Figs 3 and 4). There was a normal anatomy of the internal auditory canal on both sides. Left side of the external auditory canal was normal. Diagnosis of this anatomical malformation was compatible with congenital atresia of the external auditory canal on the right temporal region. The patient decided to proceed to surgery many years after the first diagnosis. Some weeks ago, canalplasty and tympanoplasty were performed by our surgery team. During surgery, a graft has been obtained in order to formate the covering of the new canal. The incision was made behind the ear at the level of temporal bone, and the graft needed is removed from the temporal fascia and inserted as covering of the new canal. The aim is to create a new anatomic pathway resembling a normal external acoustic canal by drilling the atretic bone and removing the present tissue (Figs 5 and 6).
Preoperative image with the atretic temporal bone.
Audiogram test.

MRI showing atresia of the right external acoustic canal.

MRI atretic temporal bone right side.

Surgical repair, formation of the new external canal.

One month post-operation.
DISCUSSION
Congenital aural atresia may be found from the early stages of life, but the time of surgical repair depends on several factors. According to the literature, congenital aural atresia refers to an anatomical malformation which mostly is presented with unilateral affection. The exact cause of congenital aural atresia is unknown and is probably multifactorial. It ultimately results from a disturbance of normal embryological development that begins as early as the sixth week of gestation, and this disorder affects the development of the first pharyngeal cleft, which is responsible for the development of the external auditory canal [3]. The most widely accepted theory is an early vascular insult of the stapedius artery, which is responsible for the development of the first and second pharyngeal arches [3, 4]. Regarding the hearing, in the unaffected side, there is normal hearing in all the frequencies, and this is different in the affected ear with a mild to moderate level of hearing loss.
Preoperative examination includes blood tests, audiogram and mostly imagistic examination. CT scan and MRI are necessary for evaluating the surrounding anatomical structures, the deformities and are quite helpful in the surgery plan. In this present case, the imagistic examination revealed unilateral mastoiditis, right atresia of the external acoustic canal and normal anatomy of the other unaffected side. According to Jahrsdoerfer grading system [4], the surgical success can be based on some clinical features regarding the profile of candidates for operation. Based on CT scan and identifying the anatomical structure, such as oval window open, middle ear space, facial nerve, malleus incus complex, mastoid pneumatization, incus-stapes connection, round window and external ear, a score is calculated, and if it is >7/10, surgical success is predicted [5, 6]. The treatment of this anatomical malformation is only surgical repair, resulting in the formation of a new bony canal resembling the external auditory one, by drilling the atretic bone and widening the closed space by removing the stenotic tissue [7]. Repair of the stenotic canal can be succeeded by anterior or posterior approach. In our case, anterior approach has been chosen. The mastoid antrum approach as and operative technique is quite reliable [8]. Removal of the stenotic and fibrotic abnormal tissue requires drilling of the atretic plate over the temporal line behind the glenoid fossa. The drilling stops at the borders of the anterior epitympanium. When the new canal is formatted, it is covered by graft. The goal is to maintain the width of new aural canal. The reconstructed auricle requires use of porous polyethylene material (MedPor) or autologous rib cartilage [8, 9]. In our patient, the auricle was repaired some years ago before the surgical repair of the atretic external auditory canal.
If left untreated, this anatomical malformation may lead to language and learning skills problems to the patient. Due to the abnormal acoustic pathway, there is also an increased risk of benign tumor formation, such as cholesteatoma, which will need surgical repair in the future. Post-operatively, there has to be a follow-up of the new graft and canal. One of the most common complications can be displacement of the new tympanic membrane and restenosis [10].
CONCLUSION
The knowledge of this anatomical malformation and its management is of paramount importance on the field of facial plastic and reconstructive ear, nose, throat surgery. Preoperative examination with MRI and CT scan is necessary in order to plan the surgical strategy. Canalplasty can a give a better esthetic result for the patient. This article refers to the case of a 56 years old patient diagnosed with congenital aural atresia in the right ear who underwent surgery of external canaloplasty and tympanoplasty but without bone conduction devices which are optional in cases with unilateral congenital aural atresia.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
The authors received no financial support for the research, authorship and publication of this article.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}