





Abstract
We describe a case of attrition rupture of flexor digitorum profundus tendon of the right little finger in a 64-year-old lady caused by a prominent hook of hamate. The tendon was reconstructed primarily by palmaris longus tendon graft and was complicated by tendon graft twisting by scar tissue, resulting in the inability to fully extend the finger.
INTRODUCTION
Attrition rupture of FDP tendon to the hamate has been reported after fractures or degenerative diseases. However, spontaneous attrition rupture caused by the hook of hamate is rare. Scarring postreconstruction of FDP tendon is common, and we describe an unusual finding at the time of reexploration for suspected tightness of the tendon graft.
CASE REPORT
A 64-year-old right-handed woman presented to our institute through the hand trauma pathway in October 2021with the inability to flex her DIPJ of the right little finger. She had forcefully tried to open a doorknob repeatedly for 20 minutes 2 weeks before the presentation.
She worked as a carer with a past medical history of asthma and hiatus hernia. She did not take steroids. She had no history of previous hand fracture or any degenerative diseases.
On examination, she had no swelling, no erythema and no tenderness. She was unable to flex her DIPJ of the right little finger; otherwise, her movement was normal. X-ray showed no fracture. An ultrasound scan was suggestive of a complete rupture of the FDP tendon within the flexor sheath.
The FDP tendon was explored under WALANT, and no tendon rupture was found within the sheath. The distal end was found in mid-palm level, and the proximal end was found in the wrist. There was evidence of attrition rupture of the FDP tendon on the very prominent hook of the hamate bone in addition to a tight carpal tunnel (Fig. 1).
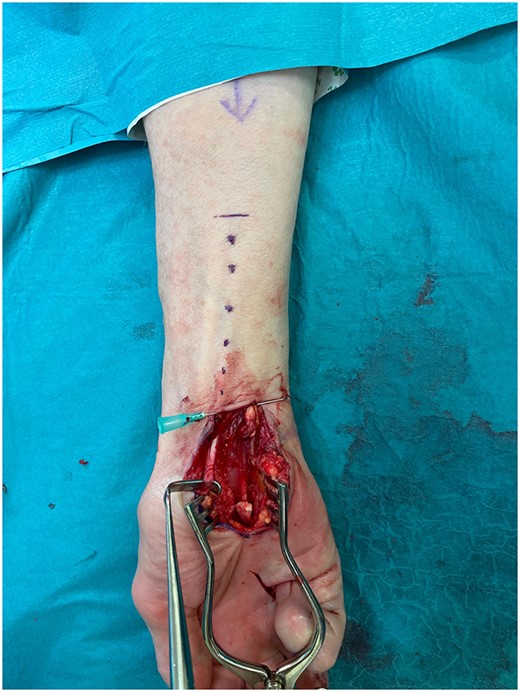
Intra-operative photo showing complete rupture of the FDP tendon with obvious gapping between the two ends.
A decision was taken for primary reconstruction by palmaris longus graft and release of the carpal tunnel. A Pulvertaft weave with 3-0 prolene was used at both ends. The repair was strong and was tested on table. The patient then was referred to hand therapy as per protocol.
She returned 8 months later to our hand clinic with a problematic restriction of full extension, which particularly affected her ability to perform yoga. When extending the finger, she was unable to fully straighten it, and after sustained exertions, the MCP extended and the PIP flexed to compensate. A tight repair was suspected, and she was scheduled for tendon lengthening.
After reexploration under local anesthesia, a longitudinal incision was done over the volar aspect of the forearm aiming at tendon lengthening by tenotomy at the musclo-tendinous junction. Three tendinous cuts were made, and the tendon looked very lax, but still the patient failed to extend her DIPJ. After consideration, the A1 pulley was released. Tendinitis was found without an apparent cause of the obstruction. The tendon graft seemed to be fully healed and functioning. Brunner incisions were used to connect the forearm to the A1 pulley incision. A bulk of scar tissue was found diverting the pathway of the tendon and acting as a pulley effect. It was changing the direction of the pull and causing this flexion deformity. Once released, the patient was able to full extend the DIPJ on table (Fig. 2; Supplementary Videos 1 and 2).
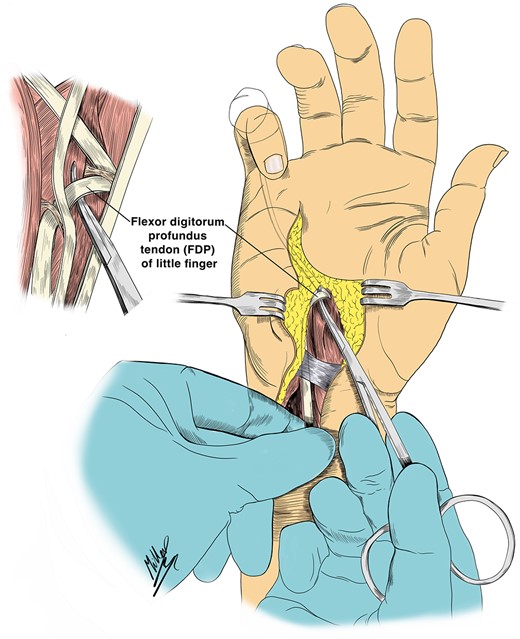
A medical illustration showing the scarring found in the second operation with change in the direction of pull of the FDP tendon acting as valve like mechanism. Illustrated by Miller Rasmy.
The patient was seen later at 1 week and 1-month post-operative with complete healing of the scar and regaining her full movement of the little finger (Supplementary Video 3).
DISCUSSION
Isolated, spontaneous rupture of FDP tendon to the little finger in non-rheumatoid patients and without history of previous fractures is rare. Our review of literature revealed six cases of attrition rupture of FDP to the hook of hamate. Three were individually reported, and the other three were reported as case series (Table 1).
A demonstration of all reported cases of attrition rupture of FDP tendon little finger caused by the hamate bone
| Paper | Case | Gender | Age | Occupation | Predisposing factor | MOI | Radiological findings | Procedure |
|---|---|---|---|---|---|---|---|---|
| Grant et al. (2005) | A | M | 55 | Builder | Nil | Manipulating motorcycle engine | Chronic non-union fracture of the hook of hamate | -Interposition PL graft -Excision of hook of hamate |
| B | M | 61 | Bricklayer | Nil | Opening a doorknob | Nil | Interposition PL graft | |
| C | M | 44 | Industrial relations officer | Piso-triquetral osteoarthritis | Gripping a loop of rope | Piso-triquetral osteoarthritis | Interposition EIP graft | |
| Jeong et al. (2012) | M | 49 | Not mentioned | Nil | Swinging the golf club | Hook of hamate fracture | -Two stage reconstruction by PL graft -Smoothening of hamate | |
| Hosokawa et al. (2016) | F | 57 | Office worker | SLE | Opening the car door | Non-union of the hook of hamate | -Tendon transfer to FDP ring -Excision of non-union hook of hamate | |
| Lee and Yeo (2016) | M | 58 | Security guard | Acromegaly | Hitting against the edge of an object | Nil | -PL graft -Smoothening of the hamate hook | |
| Our study | F | 64 | Carer | Nil | Opening a doorknob | -PL graft | ||
Three cases had underlying fracture of the hamate bone, two cases had degenerative diseases and one did not have any underlying cause and could be considered as a spontaneous rupture with an exact similar mechanism of injury to our case.
Jeong et al. (2012) [1] reported rupture to the flexors of the left ring and little fingers secondary to fracture of the hook of hamate, which was reconstructed in a two-stage operation by silicone tendon rods and then two palmaris longus grafts.
Hosokawa et al. [2] reported a similar case in 2016 of FDP of little finger rupture after insufficiency fracture in a systemic lupus erythematosus (SLE) patient. A tendon transfer was performed with excision of the hamate bone.
In the same year, Lee and Yeo [3] reported a case of FDP rupture of FDP to the little finger in addition to attrition to flexors of the ring finger in a patient with acromegaly. The rough bony edge of the hook of hamate was smoothened, and a flap of the transverse carpal ligament was used to cover the bony surface in addition to the PL graft.
In 2005, Grant et al. [4] published a case series of three attrition ruptures to the FDP little finger caused by the hamate bone.
One patient had chronic non-union hook of the hamate fracture. The second had piso-triquetral osteoarthritis. However, the third patient did not have any underlying etiology for the attrition rupture.
The author identified this patient by the letter (B). He was a 61-year-old bricklayer with no related past medical history. He reported opening a wide doorknob with the small finger while holding a wine glass stem using the remaining digits. Suddenly he felt an episode of severe pain and loss of small finger flexion.
Intra-operatively, the tendon was ruptured within the carpal tunnel. On palpation, there was a rough surface to ulnar border of the carpal tunnel over the hook of hamate with no evidence of fracture. Interpostion graft using palmaris longus tendon was used for reconstruction.
In our case, there was no history of underlying degenerative disease or evidence of hamate fracture. So, the rupture is considered to be spontaneous. We noticed an exact similar pattern to the mode of injury that was reported by Grant in his case series which was forcefully opening a doorknob.
Among the six reported cases, there were four males and two females. Three cases had underlying degenerative conditions. The mechanism of injury was almost the same in all cases; forceful wrist twisting against resistance. Two cases had a typical mode of injury; forceful opening of doorknob. Three of the six cases had an underlying fracture of the hamate bone.
The findings in the second operation was completely bizarre and unexplainable, especially that the tendon graft was intact and very strong. The scar tissue was found twisting the course of the tendon into two consecutive-90° Z-shaped manner acting as valve like mechanism when the patient tries to fully extend her DIPJ. No evidence of similar complication of twisting and scarring of the reconstructed FDP tendon was reported in literature.
CONFLICT OF INTEREST STATEMENT
The researchers claim no conflicts of interest.
FUNDING
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.

{kind=link}
{kind=link}