





Abstract
Penetrating or blunt traumas can rarely lead to renal artery pseudoaneurysms (RAPs). Renal parenchymal lacerations usually accompany them, and nephrectomy is performed in these cases. Although angioembolization of the renal artery can negate the need for nephrectomy while treating the RAP, it is not a nephron-sparing procedure. Herein, we present a case of isolated (i.e. without accompanying renal laceration) left RAP. During conservative follow-up, the RAP enlarged, and subsequently, it was treated by renal artery stent insertion. An expandable covered stent was used during this procedure. The renal function was preserved without experiencing any complications.
INTRODUCTION
Pseudoaneurysm (PA) is a disruption in the vascular wall that can lead to turbulent blood flow and hematoma formation [1]. Renal artery pseudoaneurysm (RAP) can result from penetrating or blunt trauma [2]. Because of the weakened renal arterial wall, RAP has a high risk of enlargement and rupture [3]. This study presents a case of isolated RAP developed due to a gunshot injury and treated endovascularly.
CASE REPORT
A 26-year-old male patient was brought to the emergency department due to a gunshot wound. He was hemodynamically stable; however, hematuric urine output was observed. In complete blood count, hemoglobin (Hb) and hematocrit (Hct) values were detected as 12.6 g/dl and 39.4%. The abdominopelvic computed tomography (CT) showed minimal laceration in liver segment 6, left retroperitoneal hematoma and two bullet cores adjacent to the left renal artery and lower pole of the left kidney. A CT angiography (CTA) was performed. This investigation revealed a bullet core and a 4-mm RAP in the middle of the left renal artery (Fig. 1).
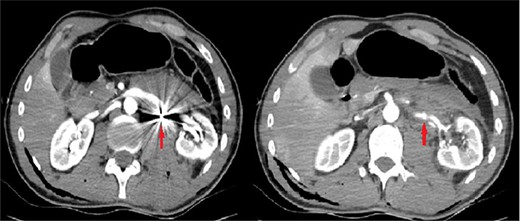
The initial computerized tomographic angiography image of the bullet core adjacent to the middle segment of the left renal artery and the renal pseudoaneurysm.
The patient was monitored; nevertheless, he started to deteriorate after a 3-h follow-up. His control Hb and Hct values were 10 g/dl and 30.1%. Despite blood transfusions and adequate intravenous hydration, the patient’s arterial blood pressure was detected as 70/50 mmHg, and his pulse rate was 132/min. An exploration was planned. During abdominal exploration, the bleeding surface of the liver was cauterized. A hematoma was observed in the left retroperitoneum. Since the hematoma did not enlarge, a conservative follow-up was planned. A surgical drain was inserted, and the incision was closed. The vital signs remained stable during postoperative follow-up.
The patient was consulted with the interventional radiology (IR) team due to left RAP on postoperative day 1. The IR team recommended the performance of a repeat CTA 1-month later. The drain was removed on the fourth postoperative day. The urethral catheter was removed after the hematuria subsided, and the patient was discharged on the 10th postoperative day.
The patient was re-evaluated with CTA 3 weeks after discharge. Endovascular intervention was planned after observing that the left RAP was enlarged to 6 mm (Fig. 2). A renal angiogram was performed. After selectively catheterizing the left renal artery, a 6 × 3 mm filling extending inferiorly in the middle part of the left renal artery compatible with RAP was observed (Fig. 3). Following catheterization of the left renal artery with a long sheath, the lesion segment was passed with guide wire-catheter manipulations. Subsequently, a 6 × 22 mm covered stent (Advanta V12 Balloon Expandable Covered Stent, AMC, USA) was placed to include the RAP neck, and full expansion of the balloon and stent was achieved (Fig. 3). The control images revealed that the RAP was excluded from circulation, and the stent was patent. No embolism or bleeding was observed in the distal renal artery branches.
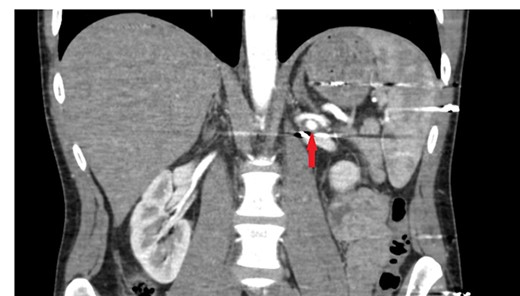
Tomographic angiography image of the enlarged renal pseudoaneurysm and the retained bullet core.
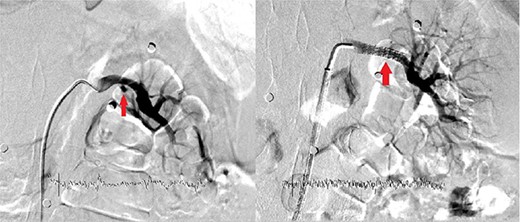
The filling image of the left renal pseudoaneurysm and the inserted covered stent.
The procedure was terminated by using a vascular closure device, which provided assurance regarding bleeding that may occur in the arterial vascular access site. During the procedure, 5000 units of heparin were given intravenously. Absolute bed rest was recommended for 24 h. The patient remained stable during this period, and no decrease in Hb value was detected. He was discharged on the second postoperative day after being prescribed clopidogrel 75 mg 1 × 1 and aspirin 100 mg 1 × 1 tablet. No RAP was observed in control CTA imaging one month after the procedure. Clopidogrel treatment was discontinued at the third-month follow-up of the patient, and he was switched to aspirin 100 mg 1 × 1 tablet. No RAP was detected in the control CTA imaging at the 6th and 12th-month control visits. Also, there was no increase in serum creatinine values, and no hypertension developed during the 1-year follow-up.
DISCUSSION
Renal artery PA can be a complication of interventions such as kidney biopsy, percutaneous nephrostomy and renal surgeries [2]. However, RAP was also reported after renal traumas [4]. Notably, penetrating traumas were associated with RAP more frequently than blunt traumas.
Although patients may present with hypertension, hematuria or lumbar pain, they may also remain asymptomatic [2]. Renal artery color Doppler ultrasonography has an essential role in the diagnosis of RAP. However, they are usually diagnosed by CT in trauma patients; CTA is the gold standard imaging method [4, 5]. The RAPs appear as round or oval structures that become opaque in the main renal artery in CTA sections [6, 7].
Although many centers recommend nephrectomy due to the risk of rupture and mortality in patients with RAP, minimally invasive treatment methods are successfully performed today [6–8]. Although some techniques include kidney embolization, others can treat the RAP and preserve kidney functions.
Lee et al. reported that they performed angioembolization to treat RAP in four patients diagnosed with renal laceration and RAP due to trauma [2]. Yamaçake et al. noted that they performed successful embolization in two patients in a case series of three patients in whom renal laceration and RAP were detected as a result of trauma [9]. They also stated that RAP disappeared in conservative follow-up after unsuccessful embolization in one patient. Although planning a conservative follow-up in our case, we performed a ‘renal artery stent insertion’ (RASI) procedure due to the enlargement of RAP.
Although the efficacy and safety of the embolization procedure in the treatment of RAP were shown in these case series, none included a patient treated with covered stent placement [2, 9]. Again, we did not find a case in which RAP developed without accompanying renal parenchymal laceration, and an organ-preserving treatment could be performed by placing a covered stent.
To the best of our knowledge, our case is the first isolated case of RAP caused by penetrating trauma, not accompanied by renal parenchymal laceration, and successfully treated by RASI and preservation of the renal function.
CONCLUSION
RASI is a safe and effective minimally invasive treatment method that prevents nephron loss in patients with post-traumatic RAP who are hemodynamically stable in terms of renovascular trauma.
CONFLICT OF INTEREST STATEMENT
The authors declare no conflicts of interest.
FUNDING
None declared.

{kind=link}
{kind=link}
{kind=link}