





Abstract
Hiatus hernia is defined as a trans-diaphragmatic protrusion of the intra-abdominal contents through the oesophageal hiatus into the mediastinum. Surgical repair is indicated in symptomatic patients, with some patients presenting emergently with strangulation and ischaemia of hernial contents. In this situation, emergent decompression and surgical repair is indicated. Although it has been suggested previously that kyphoscoliosis may contribute to development and progression of hiatus hernia, there are no published reports of obstruction being caused by severe spinal deformity. A 67-year-old male patient with spina bifida and severe scoliosis who presented with an obstructed hiatus hernia is discussed here. Because of his obstruction, laparoscopic hiatus hernia repair and fundoplication was undertaken. The patient had an uncomplicated recovery following this. This case highlights the importance of providing definitive management to patients with difficult anatomy, which has caused their obstruction, as conservative management is unlikely to lead to an optimal outcome.
INTRODUCTION
Hiatus hernia is defined as a trans-diaphragmatic protrusion of the intra-abdominal contents through the oesophageal hiatus into the mediastinum [1]. The content of a hiatus hernia is most commonly the stomach [2]. Surgical repair is most commonly indicated in patients with reflux, but also due to risk of obstruction, volvulus, strangulation of contents, and perforation; these have been well known for many decades [3, 4]. The most appropriate diagnostic imaging in an emergency presentation is computed tomography (CT), which can identify the content of the hernia, as well as strangulation [5]. The usual cause of strangulation is due to volvulus of the stomach component of the hiatus hernia, with patients describing significant chest and upper abdominal pain due to ischaemia of the strangulated organ [6].
It has previously been suggested that kyphoscoliosis (KS) may contribute to the development and progression of paraoesophageal hiatus hernias; however, this is most commonly seen in patients over 80 years of age [7]. Increasingly, the association between KS and hiatus hernia formation has been suggested due to the marked curvature of the spine leading to increased laxity of crura, widening, and disruption of the phrenoesophageal ligaments over time, leading to formation of a hiatus hernia, with patients with a greater degree of kyphosis more likely to have an intra-thoracic stomach [8]. There are, however, no published records of severe KS causing obstruction of a hiatus hernia, nor of an association between spina bifida and worsening, obstruction, or strangulation of a hiatus hernia. There are currently no uniform international guidelines for surgical technique for hiatus closure, as well as the use of mesh, with individual surgeon and institutional preferences often guiding decision-making [6].
CASE
A 67-year-old man presented to the emergency department with sudden onset epigastric abdominal pain and vomiting, on a background of a known hiatus hernia awaiting surgical management. The patient continued passing flatus but was not able to tolerate any per oral fluid intake, vomiting any intake that was attempted. Medical history was relevant for severe KS, spina bifida, reflux, recurrent urinary tract infection, and an anterior approach spinal fusion surgery. Examination was significant for severe KS, with a soft and non-tender abdominal examination. Biochemically, the patient had a very mildly raised white cell count of 12.6 † 109/l. A CT of the abdomen and pelvis was obtained that identified the progression of a known hiatus hernia in comparison with an earlier CT, containing the distal portion of the stomach. The CT showed a distended and fluid filled oesophagus and stomach, along with fat stranding around the distal stomach, concerning for obstruction and possible strangulation of the moderate hiatus hernia, along with the known severe KS (see Figs 1 and 2). A nasogastric tube was placed to decompress the stomach (see Fig. 3). Following discussion with the patient regarding their current presentation and risks of operative management, laparoscopic hiatus hernia repair and fundoplication was undertaken, which was uncomplicated, although the dissection was difficult secondary to the severe scoliosis. Intra-operatively, it was noted that the hernial sac contained a grossly dilated stomach, with all hernial contents assessed as being viable, with nil signs of ischaemia. The peritoneal sac was not resected and left in situ, with a four-stitch horizontal posterior cruroplasty undertaken, along with a 180-degree anterior fundoplication. There was concern that recovery may be complicated by respiratory failure due to the severe KS; however, the patient had no respiratory compromise, begun passing flatus, opened his bowels, and tolerated a puree diet in the days following the operation. At post-operative clinic review 4 months following the hiatus hernia repair, the patient was well, described nil issues, and was tolerating a full diet.

Axial slices of CT scan showing a moderate hiatus hernia with concern for obstruction and strangulation, with severe kyphoscoliosis.

Coronal slices of CT scan showing a moderate hiatus hernia with concern for obstruction and strangulation, with severe kyphoscoliosis.
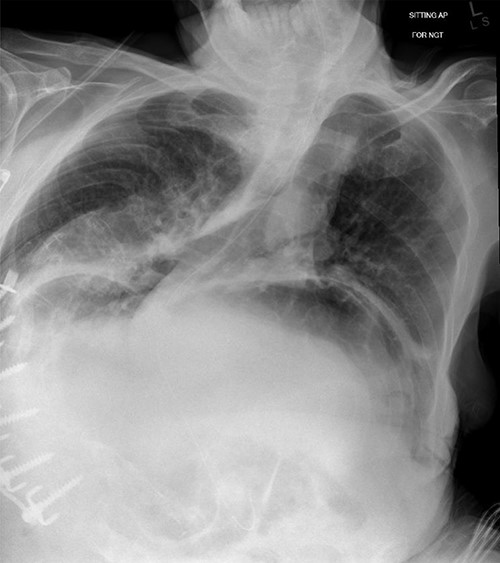
Chest X-ray showing nasogastric decompression of hiatus hernia, along with severe kyphoscoliosis.
DISCUSSION
Although prior studies have shown the possibility of progression of hiatus hernia being accelerated in patients with KS, there are no published case reports outlining, where a hiatus hernia has become obstructed in the context of severe KS and spina bifida. The mainstay of treatment in obstructed hiatus hernia or where strangulation is of concern is urgent decompression and definitive surgical repair. The anatomical causation of the obstruction of this hernia, although challenging surgically given the severity of the KS, should not be a deterrent to definitive management which will provide maximum benefit to the patient.
It is well known that KS increases in prevalence with age, with studies showing a significant proportion of patients with hiatus hernia needing repair also having KS. As populations increase in age, the prevalence of patients with obstruction of their hiatus hernia due to their KS may increase. With limited reports of other similar presentations, this case report provides an important insight into the surgical management for patients with multiple medical co-morbidities where surgery may be high-risk, and where anything but definitive repair will likely not lead to an acceptable outcome for the patient. Although this patient had an uncomplicated post-operative course, patients with severe KS undergoing hiatus hernia repair are at high-risk of respiratory complications [9]. As this patient’s severe KS is likely to worsen over time, recurrence of hiatus hernia is an important consideration in surgical repair. Although mesh repair could be considered, due to anatomical difficulties brought about by the severe scoliosis this is always a risk–benefit decision-making process as with any aspect of surgical care.
CONFLICT OF INTEREST STATEMENT
There are no conflicts of interest that require declaration.
FUNDING
The case report did not receive any funding.
CONSENT
Informed written consent was obtained from the patient who allowed for publishing of the patient history, case details and relevant imaging. This informed consent was done via telephone with another medical practitioner as witness.

{kind=link}
{kind=link}
{kind=link}