





Abstract
Mechanical intestinal obstruction is a common cause of acute abdominal pain that brings patients to the emergency department. One of the main causes is adhesion in the abdomen after abdominal surgery, but rarer causes exist and are a diagnostic challenge due to the similarity of the presenting symptoms. Here, we present a case of intestinal obstruction caused by diaphragmatic hernia.
INTRODUCTION
Mechanical intestinal obstruction is a common cause of acute abdominal pain which brings patients to the emergency department [1].
Signs and symptoms include nausea, vomiting, absence of intestinal transit, abdominal distension and bowel dilation on imaging exams. The initial approach to these patients involves symptomatic control: placement of nasogastric tube, analgesia and fluid therapy, followed by rapid diagnostic investigation. About 80% of small bowel occlusions are caused by adhesions after abdominal surgery. Other causes, rarer, are a diagnostic challenge due to the similarity of the presenting symptoms [1, 2].
The authors present a case of intestinal obstruction secondary to acquired diaphragmatic hernia.
CASE REPORT
A 62-year-old woman was admitted to the emergency department with diffuse abdominal pain starting 24 h before with gradual increase, nausea and absence of intestinal transit. She had surgical history of hysterectomy with adnexectomy and Nissen’s fundoplication. She also reports a car accident 1 year prior.
On examination, she presented: diffuse abdominal pain and tympanism on upper left quadrant and epigastrium. In rectal examination, the ampulla was empty.
The laboratory tests were normal and the abdominal X-ray showed exuberant gastric and small intestine distension and air-fluid levels.
An abdominal computed tomography (CT) scan was performed, which identified an internal hernia at the root of the right mesentery, an apparent abscess in the right lung base (65 × 55 mm) (Fig. 1) as well as elevation of the right diaphragmatic hemi-dome with Chilaiditi sign (Fig. 2).
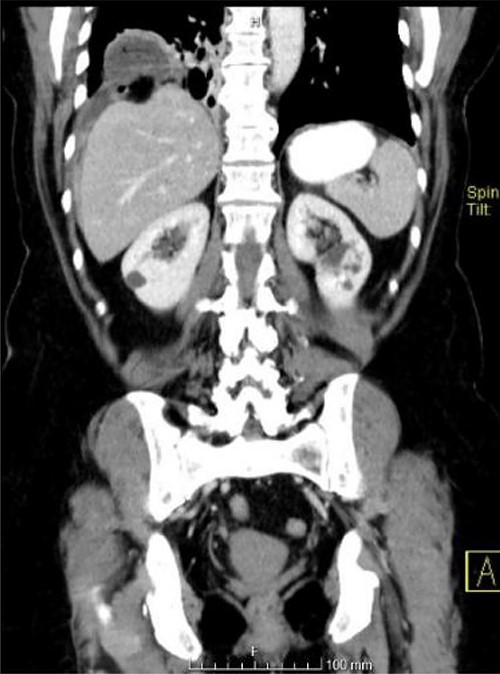
Coronal view showing a herniation of a loop to the chest.
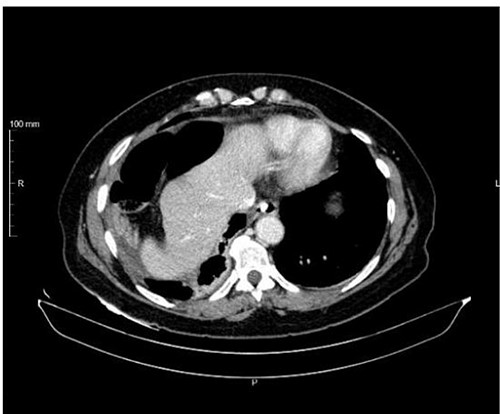
Axial view with evidence of Chilaiditi sign.
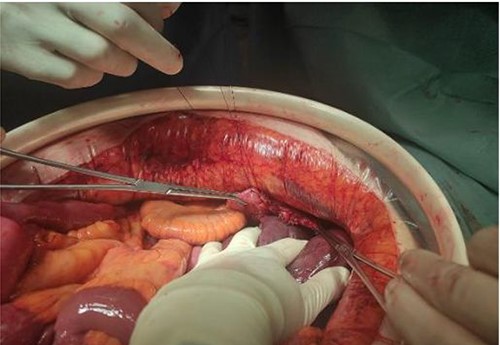
The patient underwent exploratory laparotomy, and there was a right diaphragmatic hernia with an intestinal loop in the chest. The hernia orifice was enlarged and the jejunal loop was reduced, which was necrotic without perforation (Fig. 3). Segmental enterectomy with later-lateral anastomosis was performed and a diaphragmatic repair was done with non-resorbable suture thread (Fig. 4). The abdominal and the right pleural cavities were washed and a chest tube was placed in the fifth intercostal space.

Necrotic jejunal loop.
Diaphragmatic orifice closure.
Patient developed post-operative fever, which warranted a repeat abdominal CT revealing a pelvic abscess (10 × 5.4 cm) that underwent percutaneous drainage (Fig. 5). Complete resolution was achieved, with the patient being discharged on the 20th post-operative day.

Sagittal view showing pelvic abscess; black arrow.
DISCUSSION
A diaphragmatic hernia occurs when abdominal contents cross the diaphragm to the thorax. This entity can be congenital or acquired. Of the acquired, mostly are secondary to trauma and are four times more common in males. Spontaneous diaphragmatic hernia is very rare. Still, it is thought that these hernias may be secondary to a remote trivial trauma or a small congenital defect. They are more common on the left side; this is partly due to protection offered by the liver and partly because of fusion defects that occur in the embryonic period [3].
Diaphragmatic hernias may go unnoticed on initial imaging exams. Only 25–40% of radiographs taken on admission are diagnostic, and CT scan is an accurate help [4].
In an acute phase, the treatment of intestinal occlusion due to incarcerated diaphragmatic hernia requires respiratory and circulatory resuscitation. Even so, because it is potentially life-threatening, surgery is the treatment of choice in most cases [3, 5].
Usually, when an acquired diaphragmatic hernia is diagnosed after a recent history of trauma, laparotomy is performed by an abdominal approach. However, if the diagnosis is made incidentally, after months or years of trauma, most surgeons prefer the thoracic or thoracoabdominal approach. This approach seems better in case the hernia content has adhered to the thoracic structures. In this case, we choose to close the hernia defect directly without any tension. Currently, the use of pledgeted interrupted mattress sutures is defended, and in some cases, the diaphragm can be sutured to the intercostal muscles or around the ribs [3].
The death rate depends on co-morbidities and is very variable (5–50%), and recurrence occurs in a small number of patients. It is suggested that diaphragmatic injuries be diagnosed before the complications, like diaphragmatic hernia and strangulation of the abdominal viscera in the thoracic cavity (as we show in this case), because the mortality and morbidity increase. In the literature, the most common incidence of delayed diagnosis was the right-sided diaphragmatic rupture [3].
CONCLUSION
This case report shows us that intestinal occlusion, very common in an emergency context, can have a complex cause. The clinical history can help in the diagnostic suspicion and the CT scan is essential to confirm and characterize the defect. Correct diagnosis and early treatment are essential for success.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}