





Abstract
Meckel’s diverticulum (MD) is the most common congenital malformation of the gastrointestinal tract. The most frequent complications are bleeding, intestinal obstruction, intussusception and neoplasm. Perforation because of diverticulitis is very rare and usually associated to foreign bodies. We report a case of an elderly man who presented with right iliac fossa pain, raised inflammatory markers and a computer tomography (CT) scan suggestive of Meckel’s diverticulitis. He underwent a laparoscopic converted to open small bowel resection and primary anastomosis for perforated MD, which revealed a corn kernel at its base in the absence of ectopic gastric or pancreatic tissue. Symptomatic and perforated MD secondary to a phytobezoar is extremely rare in elderly patients, hence the importance of clinical suspicion in patients with abdominal pain, independent from their age, to avoid delay in diagnosis, which can lead to increased morbidity and mortality in this demographic.
INTRODUCTION
Meckel’s diverticulum (MD) is a relatively common abnormality of the gastrointestinal tract due to incomplete obliteration of the omphalomesenteric duct, which normally obliterates within the first 9 weeks of gestation. It is a true diverticulum, containing all three layers of the bowel wall and it arises from the antimesenteric border.
MD occurs in about 2% of the population, clinical presentation is usually before the age of 2 and is found twice more common in males than in females [1]. Symptomatic MD range from 4–16% [2], with the most common presentation being intestinal obstruction, gastrointestinal hemorrhage and inflammation [3]. Perforation of MD by foreign bodies is unusual as they tend to pass through the gastrointestinal tract without consequences [4].
The following case is an interesting and very rare presentation of perforated MD due to a corn kernel in an elderly patient.
CASE REPORT
A 77-year-old male presented to the Emergency Department with a 2-week history of progressive colicky right iliac fossa (RIF) pain and abdominal distension. 48 hours prior to his hospital presentation, the pain worsened, becoming generalized, constant and associated with subjective fevers, diarrhea, nausea and one episode of bilious vomiting.
His medical background included hypertension, hyperlipidaemia, paroxysmal atrial fibrillation, benign prostatic hyperplasia and bilateral inguinal hernia repairs.
On examination, he had normal observations, his abdomen was distended, bowel sounds were present with tenderness and localized guarding of RIF and suprapubic area. His blood tests showed an elevated white cell count and C-reactive protein, 17.2 × 10^9/L and 186 mg/L, respectively. He subsequently had a computer tomography (CT) (Fig. 1), which showed a blind-ending tubular structure in the RIF arising off the ileum that measured 5 cm in length and contained fecalized material within the tip associated with extensive adjacent stranding of the mesentery consistent with acute Meckel’s diverticulitis. The appendix was normal.
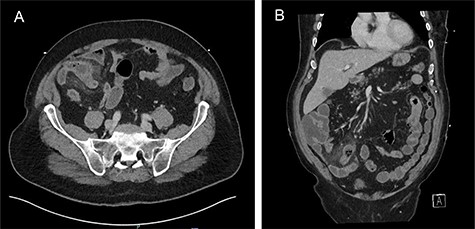
(A) Axial and (B) coronal views: acute Meckel’s diverticulitis in RIF associated with extensive adjacent mesenteric stranding.
He was commenced on intravenous antibiotics and underwent an initial laparoscopy where an inflamed MD with local perforation was found with significant surrounding inflammation, a normal appendix was confirmed (Fig. 2). The decision was made to convert to a mini-laparotomy given the need for a small bowel resection with subsequent stapled side to side anastomosis. On macroscopic examination of specimen in the operating theater, a corn kernel was found obstructing the lumen of the diverticulum.
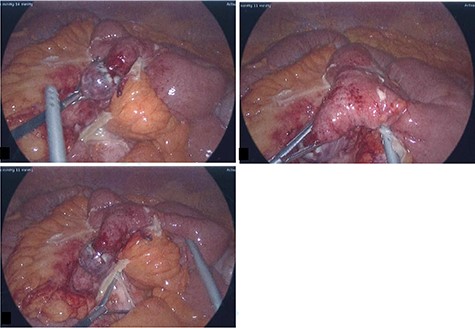
Intra-operative photos: acutely inflamed MD with a wide base and gangrenous tip, associated with significant surrounding inflammation.
The histology confirmed a small bowel diverticulum with no ectopic gastric or pancreatic tissue within it, full-thickness gangrenous necrosis of the wall with secondary perforation, abscess formation within the peridiverticular mesentery and acute fecal peritonitis. Fragmented vegetable material consistent with a seed of corn present within the distal diverticular lumen in the region of the perforation was reported.
DISCUSSION
MD is a true diverticulum that contains all three layers of the bowel wall. Less than 10% of cases are diagnosed prior to surgery [5], MD is often found incidentally during a surgical procedure.
There are multiple risk factors that have been associated with an increased risk of developing symptomatic MD, including male sex, diverticulum >2 cm in length, presence of ectopic tissue and age <50 [6].
Meckel’s diverticulitis can be difficult to distinguish clinically from other more common causes of abdominal pain such as appendicitis, diverticulitis, inflammatory bowel disease or bowel obstruction.
CT has become a valuable resource for the investigation of abdominal pain and Meckel’s diverticulitis can be identified as a blind-ending tubular structure associated with inflammatory changes of the surrounding mesentery and bowel wall. These findings helped to obtain the patients diagnosis prior to surgery in our case.
Diverticulitis is seen in 13–31% of complicated cases of MD [7]. Perforation is very rare and is responsible for 0.5% of symptomatic MD [8, 9], mainly related to foreign bodies, inflammation and trauma. There are multiple foreign bodies that have been reported as a cause of perforation of MD with fish bones accounting for 55% of the cases in one of the studies. Surprisingly, objects like rolled tomato skin and cabbage stalks were also found as a cause of perforation [10]. After extensive literature review, this is the first case of MD perforation secondary to a corn kernel. The pathogenesis could be explained mainly by two reasons: firstly, by local inflammation due to irritation of the foreign body against the wall of the diverticulum and secondly, due to peristalsis in attempt to push the foreign body to the tip of the diverticulum. Both could lead to a decrease in blood supply, necrosis, perforation, localized peritonitis and abscess formation as seen during surgery and confirmed by histology [11]. The characteristics of the foreign body involved in our case, being a soft corn kernel, might explain the long duration of symptoms with 2 weeks of inflammation preceding necrosis and perforation 48 hours prior to presentation to the emergency department.
In several surgical series, the average mortality of MD has been reported at around 6%, with a large proportion of deaths occurring in elderly people [12].
This case is a rare finding as the incidence of symptomatic MD decreases with age, perforation is present in <1% of complicated MD, and food is a very uncommon cause for it. In addition, the fact that there was no presence of ectopic tissue reinforces the hypothesis that the perforation of the MD was secondary to a foreign body.
CONCLUSION
Although perforation of MD is rare, a missed diagnosis could lead to fatal consequences. Early suspicion and recognition are required for appropriate surgical management. The case report presented a rare complication in an elderly patient of MD perforated by a seed of corn, highlighting the importance of considering MD and their rare etiologies as a cause of acute abdomen even in the elder population.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}