





Abstract
Few articles have reported cases of perianal abscess due to ingested foreign bodies. Herein, we report a case of perianal abscess due to a long fish bone.
A 72-year-old man who was toothless and wore a denture had a chief complaint of anal pain. His left-side buttock had swelling and redness. Computed tomography revealed a perianal abscess on his left-side buttock and high-intensity linear structure in the abscess cavity. We made a diagnosis of perianal abscess due to a fish bone and performed an emergency operation. We opened the abscess cavity and removed the 5 cm fish bone from the cavity. After drainage of the abscess cavity and antibiotic administration, he was discharged from our hospital on day 8.
A long fish bone could cause perianal abscesses. Rapid diagnosis and ensuring fish bone removal are important to prevent sepsis.
INTRODUCTION
Ingested foreign bodies are known to cause gastrointestinal perforations [1, 2]. However, perianal abscess due to ingested foreign body is rare [1, 3]. Previous studies reported cases of perianal abscess due to ingested foreign bodies. Table 1 shows the cases of perianal abscess due to ingested foreign bodies found in a PubMed search (Table 1) [3–7]. Perianal abscess due to foreign bodies was considered to cause penetrating anal canal and perianal tissues [5]. The foreign bodies that caused perianal abscess were short (Table 1), and only few cases of perianal abscess due to long foreign bodies have been reported. Herein, we report a case of perianal abscess due to an ingested long fish bone.
Cases of perianal abscess due to ingested foreign bodies
| Author | Type of foreign body | Number of patient | Size (cm) |
|---|---|---|---|
| Liu et al. [3] | Jujube pit | 2 | 3 |
| Kocierz et al. [4] | Pig bone | 1 | 3 |
| Doublali et al. [5] | Lamb bone | 1 | 3 |
| Delikoukos et al. [6] | Fish bone, chicken bone, toothpick and pin | 4 | 2–3 |
| Seow et al. [7] | Fish bone | 6 | 2–3 |
| Our case | Fish bone | 1 | 5 |
CASE REPORT
A 72-year-old man who had type 2 diabetes and was toothless visited our hospital because of anal pain that had started a week before. Swelling and redness were observed on his left-side buttock. Digital examination revealed swelling of the left-side anal canal. The blood examination test result showed elevated white blood cell count and C-reactive protein level. The computed tomography (CT) revealed a fluid cavity containing air in his left-side buttock and a high-density linear structure in the cavity (Fig. 1a). Furthermore, we found several linear structures in the gastrointestinal tract (Fig. 1b). We made a diagnosis of perianal abscess due to a foreign body and performed an emergency operation. We especially suspected a foreign body, particularly a fish bone, in the abscess cavity on the basis of the CT scan findings.
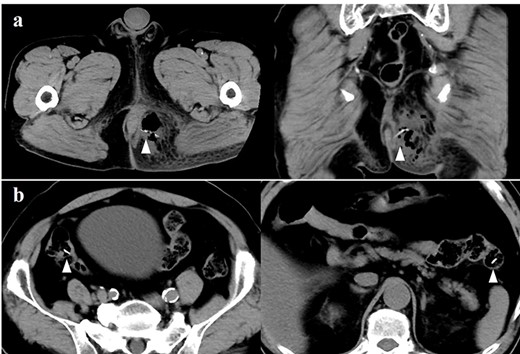
(a) A computed tomography scan showing the perianal abscess cavity containing air in the left-side buttock. The arrow indicates the fish bone in the abscess cavity. (b) Several high-intensity structures (white arrow) suspected as fish bone in the gastrointestinal tract.
We performed an operation under lumbar anesthesia in the jackknife position. We cut on the swollen site on the left-side buttock and drained purulent discharge. We also found and extracted from the abscess cavity foreign bodies, including the fish bone, which were detected on the preoperative CT scan. The foreign body was 5 cm long (Fig. 2). We irrigated the abscess cavity with saline and placed an 8 mm Penrose drain. We did not close the wound to drain discharge after the surgery. The bacterial culture of the sample taken from the abscess cavity showed Escherichia coli. Accordingly, the patient received tazobactam/piperacillin until day 3 and clavulanic acid/amoxicillin between days 4 and 11. In the postoperative course, the amount of discharge from the drain decreased day by day. The findings from the buttocks and the white blood cell count and C-reactive protein level were improved. The drain was removed on day 6, and the patient was discharged from the hospital on day 8. After the operation, the patient remembered that he ate fish (barracuda) before the onset of his symptoms and ate food without his denture because it would not fit his mouth.

The 5 cm fish bone removed from the abscess cavity.
DISCUSSION
In our case, a long fish bone caused a perianal abscess. Table 1 shows that the length of foreign bodies which were reported as a cause of perianal abscesses ranged from 2 to 3 cm. It is considered that a long ingested foreign body is usually difficult to reach to anal canal. However, the length of the fish bone in our case was 5 cm, which is the longest among the other foreign bodies reported as cause of perianal abscess previously. Our case suggests that a long fish bone could reach the anus without penetrating into the gastrointestinal tract and cause a perianal abscess similarly to short foreign bodies.
Preoperative diagnosis is crucial in the treatment of perianal abscess related to ingested fish bones. The reason is that diagnosis of the size of the abscess cavity and length, location and number of fish bones before operation is important for ensuring the removal of fish bones. Kocierz et al. reported that they detected a pig bone in the perianal abscess cavity on radiography [4]. However, in our case, we did not detect fish bones on radiography because the fish bone was thinner than a pig bone (data not shown). Bernard et al. [8] reported that ingested fish bone was shown as a linear and high-density object on the CT scan. Thus, we considered the CT scan to be an adequate diagnostic modality for perianal abscesses due to ingested fish bones.
From the viewpoint of the treatment, ensuring the removal of the ingested bones, an open abscess cavity, and rapid drain discharge was important. Thus, we considered that local anesthesia was insufficient for the extraction of the fish bones and lumber anesthesia was needed for this case. This strategy was similar to the previously reported cases [4, 5]. We administrated antibiotics for 11 days in this case. Leung et al. [9] reported that antibiotics were not always required for perianal abscess or systemic sepsis. On the other hand, Shimizu et al. [10] reported that ingested bones caused Fournier’s gangrene and sepsis. Our patient did not have Fournier’s gangrene and sepsis. However, he had type 2 diabetes, which was reported previously as a risk factor of Fournier’s gangrene [11]. Therefore, for patients at high risk of Fournier’s gangrene, we considered quick drainage and administration of antibiotics for gram-negative bacilli and anaerobic bacteria necessary to avoid progression to sepsis.
Moreover, the patient had no teeth and took food without his denture before the onset of his symptoms. Arulanandam et al. [12] reported that denture wearing was a risk factor of gastrointestinal perforation due to fish bones. Similarly, in this case, we detected a long fish bone in the abscess cavity and several foreign bodies in the gastrointestinal tract, including a fish bone, on the CT scan. These findings suggest that the patient could not chew food including fish bones enough. Therefore, we considered that toothless or denture-wearing patients might be at risk of perianal abscess due to fish bones, and adjustment of denture or dietary guidance could prevent recurrence.
In conclusion, we consider that long fish bones could cause perianal abscesses. Rapid diagnosis and ensuring fish bone removal are important to prevent sepsis. Furthermore, toothless or denture-wearing patients might be at risk of perianal abscess due to fish bone.
AUTHORS’ CONTRIBUTIONS
T.I. collected the clinical data. All authors critically revised the manuscript and approved the final version to be published. All authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
None.
INFORMED CONSENT
Informed consent was obtained from the patient in this case.

{kind=link}
{kind=link}