





Abstract
Retention of an intercostal drain segment is an uncommon and infrequently reported complication of underwater seal drain use. We report the case of a 66-year-old New Zealand European male who underwent bilateral lung transplantation for severe chronic obstructive pulmonary disease and bronchiectasis. The patient required a return to the operating room for exploratory surgery after an intercostal drain severed during its attempted removal and became retained within the chest cavity. A deep suture had inadvertently been passed around the chest drain intraoperatively. In the event of such a complication, prompt recognition and removal of the retained segment is required. This novel case is reported to highlight the possibility of an entrapped suture as a cause of resistance when attempting to remove an intercostal drain. Kinking on a chest X-ray may also point to this problem, and senior input should be sought early if radiographic findings are coupled with clinical difficulties.
INTRODUCTION
Underwater seal drains are safe and commonly used instruments in many cardiothoracic surgical procedures [1]. Retained chest drain segments are rare complications but [2], when they do occur, require urgent recognition and same-day surgical removal to reduce pain and the risk of pulmonary laceration [2–4]. We report the case of a patient who was returned to the operating room for exploration of the chest cavity after an intercostal drain was fractured and retained within the chest cavity during its attempted removal.
CASE REPORT
A 66-year-old New Zealand European male was admitted to the hospital to undergo elective bilateral lung transplantation for severe chronic obstructive pulmonary disease and bronchiectasis. The patient’s past medical history included lifelong asthma, occupational exposure to flour dust and a 50-pack-year history of cigarette smoking.
A clamshell incision was performed to enter the pleural spaces and the sternum was then divided with an oscillating saw. Sequential lung transplantation was then performed routinely and uneventfully. Towards the end of the case, 28 French chest drains (Smiths Medical, Minneapolis, MN) were positioned within the apical and basal regions of each hemithorax (Fig. 1). To close, 1-0 Vicryl (Ethicon Inc, Bridgewater, NJ) sutures were applied to the pericostal layer in a figure-of-eight manner and wires were applied to the sternum. Further Vicryl sutures were applied in layers to close the deep tissue and skin. The patient was transferred to the intensive care unit in a stable condition. Ventilatory, inotropic and vasopressor support was weaned off on Day 1, post-operatively. Both apical chest drains were removed without incident on Day 2, and the patient was transferred to the ward.

Chest X-ray demonstrating placement of the four chest drains.
The left basal chest drain was removed without incident on Day 5. However, the nurse encountered resistance during attempted removal of the right basal chest drain. The intern was subsequently notified. Resistance was also encountered by the intern during a further attempt to remove the chest drain. A chest X-ray performed earlier in the day was reviewed (Fig. 2). It demonstrated kinking of the drain around a rib. The intern altered the direction of traction in order to account for the kinking but, during gentle traction, the chest drain fractured at the 14-cm mark (Fig. 3) and became retained within the right hemithorax (Fig. 4). The thoracostomy wound was closed and senior help was immediately sought.
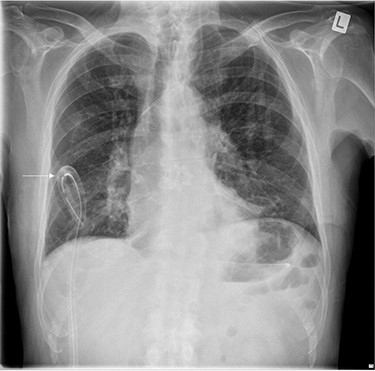
Chest X-ray demonstrating kinking of the chest tube around a rib on the right side.

A 28 F chest tube that became severed at the 14-cm mark upon attempted removal.
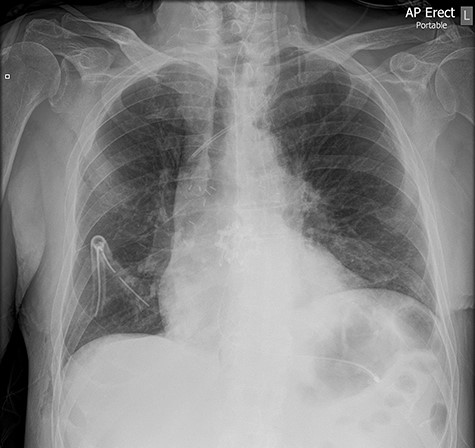
Chest X-ray demonstrating the retained chest tube segment on the right side.
The patient was returned to the operating room several hours’ later for exploratory video-assisted thoracoscopic surgery and the retained chest drain segment was removed. It was observed that a 1-0 Vicryl pericostal suture had passed around the tubing at the time of chest closure, thereby securing the 14-cm chest drain fragment against the internal chest wall. The patient’s post-operative recovery was otherwise uneventful and he was routinely discharged from the hospital on Day 18. The incident was reported to the Health Quality and Safety Commission of New Zealand.
DISCUSSION
Iatrogenic retention of an intercostal drain segment is an unusual complication of chest drain use [1], which causes pain and potentiates neurovascular injury and pulmonary laceration. When it occurs, it almost always requires reoperation for foreign body removal, with or without decortication [2–4], which exposes the patient to an extra general anaesthetic [1–3, 5, 6] and can prolong hospital stay. Video-assisted thoracoscopy is a reasonable approach because foreign bodies may be easily removed while avoiding open surgery [7].
Our patient experienced significant pain when the chest drain segment became retained within the chest cavity. In such an event, it might be appropriate to consult the anaesthetic team for pain management while fasting the patient for a general anaesthetic. If the patient is physiologically unstable, vascular injury or pulmonary laceration might be the cause, and emergency exploration should be undertaken. In the event of cardiac arrest, a rescue thoracotomy should be performed in case cardiac laceration has occurred.
Several cases of chest drain retention have been reported [1–6, 8, 9]. Drain tip dislodgement complicated a Seldinger approach in one case [2], probably as a result of the repeated to-and-fro action over the guide wire while, in another, a Penrose drain was accidentally lost within the pleural cavity during open window thoracostomy [3]. Although the cause of damaged tubing was not identified in a patient treated for a retained segment of a Pleurocath [1], an oblique line was observed between the two eyes of the drain at the 7-cm mark upon its removal, possibly indicating a shearing-type mechanism. A similar shearing effect was documented in two other reports: in one, a Bonanno catheter tip fractured [8] and, in another, negligent removal caused tearing of the drain [3]. A retained chest drain segment was reported on computed tomography (CT) scan in yet another case but was later identified as being a calcified track without iatrogenic chest drain retention [9].
Despite the various causes of chest drain retention that have been reported [1–6, 8], we have not identified a case in which a drain became severed because of suture entrapment. It is probable that similar cases exist but are unreported. The deleterious consequences of a retained chest drain fragment emphasize the importance of raising awareness about this perioperative complication [1].
Our case serves as a reminder to be mindful of intercostal drain entrapment when placing pericostal sutures. The possibility of inadvertent suture entrapment of a chest drain as a differential diagnosis to kinking observed on a chest X-ray is also highlighted.
Senior input should be obtained if significant resistance is encountered during the removal of a surgical chest drain, especially when coupled with radiographic findings of drain distortion. Doing so may prevent chest drain fracture and unnecessary patient discomfort while surgical exploration is awaited.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
None.

{kind=link}
{kind=link}
{kind=link}
{kind=link}