





Abstract
Angioleiomyomas are relatively rare benign soft tissue tumors which often occur in the extremities. The true etiology is largely unknown and is seldom associated with pain. They are rarely diagnosed preoperatively as the clinical and radiological examinations are often nonspecific and inconclusive. The patients may face a considerable delay before a specialist treatment is sought due to the varied presentation/missed diagnosis preoperatively. This delay highlights the need for better characterizing the diagnosis and treatment of angioleiomyomas in clinical setting to expand awareness of this pathology, the differential diagnosis of lower extremity soft tissue tumors and the need for ongoing publication of such case reports. We wish to present two patients who came in with foot and ankle swellings and heel pain. Post-excision, these swellings were histologically diagnosed as benign angioleiomyomas.
INTRODUCTION
Angioleiomyomas or vascular leiomyoma, are smooth muscle tumors, which arise from the tunica media (smooth muscle layer) of the subcutaneous blood vessels [1, 2]. They account for ~4.5% of all being soft tissue tumors [3] and 0.2% of benign foot lesions. Angioleiomyomas typically present as a firm, rounded mobile nodule arising from deep layers of dermis/subcutaneous tissues. They are slow-growing masses that can be asymptomatic but often present with pain, discomfort, nerve entrapment or causing patient concerns with footwear or cosmesis. The majority of angioleiomyomas are small (0.5–2 cm in diameter). Due to their rare occurrence, lack of clinician awareness and paucity of published literature, they are rarely diagnosed preoperatively. An accurate diagnosis can prevent delays in treatment, improve the outcomes and also help in excluding the involvement of malignancies. Enhancing the general awareness of angioleiomyomas in clinical practice will improve its treatment outcomes. We wish to present two cases that presented as painful swelling over the foot and ankle, which were diagnosed as angioleiomyomas after excision and histologic examination.
CASE REPORT 1
A 34-year-old gentleman presented with a swelling over the posterolateral aspect of his right ankle close to the Achilles tendon. He complained of pain and sensitivity to wearing shoes. The swelling was 10 × 5 mm, mobile and ultrasound (US) scan reported it as ‘A well-defined ovoid hypoechoic lesion underneath the skin surface measuring approximately 11 mm × 3 mm in diameter and appears related to a linear hypoechoic structure’ (Fig. 1). ‘The lesion is slightly heterogeneous in texture and shows posterior acoustic enhancement on the underlying tissues. There is mild internal vascularity of this lesion on Doppler assessment’ (Fig. 2) and ‘these appearances are suggestive of superficial neuroma lesion’. Post-excision, the histology of a single piece of pale smooth firm tissue (9 × 6 × 5 mm) was reported as angioleiomyoma. He made an uneventful recovery and was discharged after 4 months of follow-up.
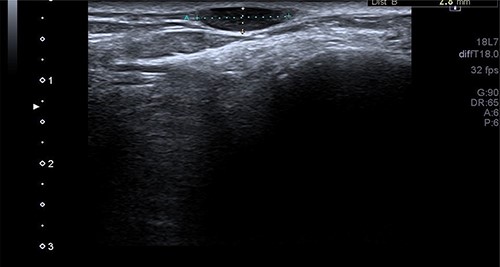
The US scan image of the right ankle posteriolateral aspect of Patient 1, which showed a well-defined ovoid hypo echoic lesion underneath the skin surface; measuring ~11 × 3 mm in diameter.

The Doppler US image of the right ankle posterolateral aspect of Patient 1, which shows mild internal vascularity.
CASE REPORT 2
A 50-year-old lady presented to us with a lump in her left foot on the lateral aspect at the level of the calcaneocuboid joint for a 1-year duration, which was associated with pain. She consulted her GP who advised an US scan. This revealed a lump over the dorsum of the left foot on the lateral side. She also had a magnetic resonance imaging (MRI) scan which was indeterminate (Figs 3 and 4). It was reported as a suspected sarcoma. She was then referred to the Sheffield sarcoma unit where she underwent a biopsy of the swelling; which was reported as angiomyolipoma (a benign swelling). She was not keen on excision initially, but as the swelling increased in size and started becoming painful, she underwent an excision of the lesion under our care and the histopathologic examination of the excised sample confirmed it to be angioleiomyoma. The post-operative period was uneventful and she was discharged from our care after 10 weeks. At this time, she was symptom-free and had a pain score of 0/10.

T1 MRI image of the soft tissue lesion over the lateral foot in Patient 2, which shows a lesion isointense to hypointense to the muscle.

T2 axial MRI image of the soft tissue lesion over the lateral foot in Patient 2 showing a lesion which is heterogeneous and slightly hyperintense to the muscle.
DISCUSSION
Angioleiomyoma is one of the three different forms of leiomyoma, which is also known as vascular leiomyoma. The other forms of leiomyoma include piloleiomyoma (arising from arrestor pili muscles) and genital leiomyoma (arising from the smooth muscles of the scrotum, vulva or nipple). Angioleiomyoma is uncommon and benign. Its etiology is largely unknown but factors such as trauma, infection, hormones and arteriovenous malformations have been known to be present in various cases [4]. Histologically, they have a well-circumscribed dermal nodule surrounded by a compressed connective tissue and separated from it by clefts. Various sized veins with muscular walls are present within the nodule, and smooth muscle bundles extend tangentially from the periphery of the vessels. The lumina of the veins is rounded or slit-like and has a minimal amount of collagen [5]. Frequently, they occur in extraosseous tissues such as ovaries, lungs, uterus, bladder and GI tract [6]. It is more prevalent in women than in men with a ratio of 2:1 and affects the middle-aged population mostly. About 50–70% are found in the lower limbs [7]. Differential diagnoses can include lipoma, fibroma, ganglions, schwannoma, cutaneous angiolipoma, glomus tumor, etc. [4].
Pain is not always present, but if present, can be of varied character—pressure pain, sharpness or pinching type and is affected by temperature [2]. This pain has been hypothesized to be a result of local tissue anoxia or due to compression of the local neural structures [7]. In our case series, both the patients presented with painful swelling and there was no distal neurovascular involvement.
An arteriogram or Doppler study may be useful to an extent, but a confirmed diagnosis is only obtained through histopathological examination after excision [8–10]. Case 1 had an US scan of the swelling which showed a well-defined ovoid hypoechoic lesion underneath the skin surface, and the lesion was slightly heterogeneous in texture and shows posterior acoustic enhancement on the underlying tissues. There was mild internal vascularity of this lesion on Doppler assessment—appearances suggestive of superficial neuroma lesion. The usual appearance of these lesions on USS is a well-circumscribed oval mass with a homogenous echotexture and occasionally hypoechoic protrusions.
Similarly, in Case 2, the patient had an MRI scan which reported an indeterminate swelling suggestive of a possible sarcoma. As the MRI findings were not characteristic of the MRI findings of an angioleiomyoma, such as T1: isointense or hyperintense to muscle, T2: heterogeneous and slightly hyperintense to muscle and T1 C+ (Gd): homogenous to heterogeneous enhancement, suspicion of the sarcoma was reported from the MRI scan findings and referral to sarcoma unit was advised. This clearly shows that the US and the MRI scan findings can suggest a different diagnosis, and a confirmed diagnosis was only established following excision and histopathological examination of the excised lesion. Usually, angioleiomyomas have a peripheral low-intensity signal rim corresponding to a fibrous pseudo capsule with adjacent vascular structures with isointense or hypointense to muscle on T1 images and heterogeneous and slightly hyperintense to muscle on T2 images.
Simple excision and biopsy is the best treatment, but the decision to proceed with surgery depends on the site and size of the lesion as well as the severity of the symptoms. In our case series, both the patients had simple excision of the lesion with complete resolution of the symptom following the excision. After excision, malignant recurrence is extremely rare. Complications, such as secondary calcification, myxoid degeneration, hyalinization and malignant transformation, were reported [6]. In case of recurrence, it has been discussed that the new lesion must be removed and treated like other low-grade malignancies [3].
CONCLUSION
Angioleiomyoma is a relatively uncommon benign subcutaneous soft tissue mass which most often occurs in the extremities. They are often misdiagnosed and a degree of suspicion should be maintained in patients presenting with growing soft tissue tumors in the lower extremities. Simple excision and histopathology are recommended, especially when associated with pain or difficulties associated with the protruding mass. Imaging can be of assistance in visualizing the mass and its surrounding structures before surgical excision.
CONFLICT OF INTEREST STATEMENT
We declare that we have no conflict of interest in publishing this article.
FUNDING
We did not receive any funding for this article.

{kind=link}
{kind=link}
{kind=link}
{kind=link}