





Abstract
A report of true aneurysms is extremely rare. There are only five previous case reports of true aneurysm of the facial artery. In the previously reported cases, there was no case that underwent trapping and surgical excision. In this case report, we describe the procedure of internal trapping before the surgical excision of a huge true aneurysm of the right facial artery for a 79-year-old woman. There was no recurrence of the aneurysm during a 6-month follow-up period.
INTRODUCTION
Aneurysms are localized swellings of the arterial wall in some parts of the body and are classified into true and false types. A true aneurysm refers to the enlargement of the vessel wall structure without traumatic injury. It involves all three layers of the arterial wall (intima, media and adventitia). Reports of true aneurysms are uncommon, especially aneurysms of the facial artery that branches from the external carotid artery is extremely rare. In this case report, we describe the procedure of internal trapping before the surgical excision of a true aneurysm (5 cm in diameter) of the right facial artery for a 79-year-old woman. This is the first case surgical excision of the true aneurysm after internal trapping. Furthermore, we provide a literature review of the cases of true aneurysms of the facial artery.
CASE REPORT
A 79-year-old female non-smoker presented with painless swelling below the left side of the mandible angle, which was first noticed 4 years previously (Fig. 1). She had no history of cardiovascular disease, diabetes mellitus and trauma to the head and neck. The palpable mass was pulsatile and had a diameter of 5 cm. Intraoral examination was unremarkable. A computed tomography (CT) (Fig. 2) and a magnetic resonance imaging scan demonstrated the presence of a 5-cm left submandibular gland tumor, whereas contrast-enhanced CT (Fig. 3) and ultrasonography revealed a 3.8 × 3.3 cm aneurysm of the facial artery with a cystic structure. We judged a submandibular tumor with pseudoaneurysm or a true aneurysm and suggested treatment options for the mass. The patient selected surgical excision under general anesthesia in response to the pathological diagnosis and to ensure the recovery of her esthetic appearance. We, therefore, consulted endovascular surgeons for angiography and internal trapping before the surgical excision, considering that there was a risk of bleeding during the operation.

Photograph of the left submandibular mass.
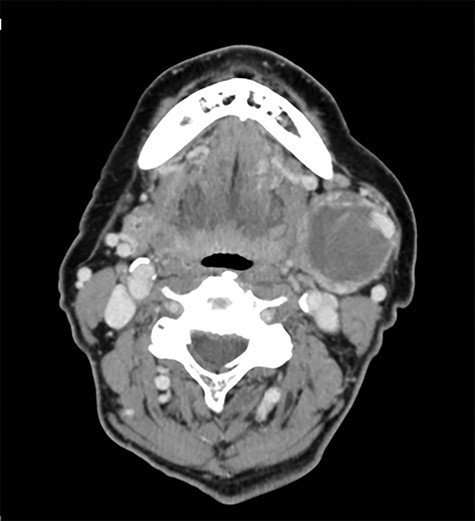
Preoperative axial enhanced computed tomography image.

Preoperative contrast-enhanced computed tomography with 3D reconstruction.
A parent vessel occlusion was performed with coils by endovascular surgeons from the distal to the proximal side of the aneurysm under local anesthesia (Fig. 4). After the endovascular trapping with coils, the facial mass was non-pulsatile.
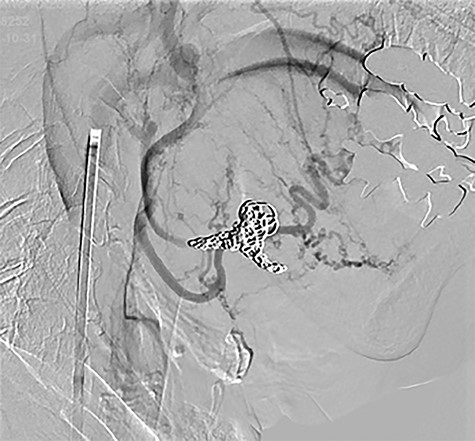
Postoperative trapping with coil.
A total of 8 days after the internal trapping, the patient underwent an operation for excision of the aneurysm under general anesthesia. Skin incision was made using the submandibular approach at 4-cm below the inferior border of the mandible, thus exposing the facial artery and the aneurysm. The mass adhered to a left submandibular gland and the gland did not have any structural change. We, therefore, isolated and saved the gland from the mass. Subsequently, we ligated the facial artery and excised the mass, and then closed the skin using a 5-0 nylon suture (Figs 5, 6). The histopathological examination of the excised mass confirmed a true aneurysm of the facial artery with organized thrombus. There was no bleeding from the wound during or after surgery. The postoperative course was uneventful; the patient had no facial nerve palsy and there was no recurrence of the aneurysm during a 6-month follow-up period.
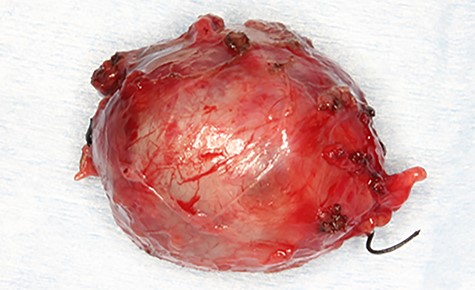
Photograph of the removed aneurysm. The coil was found in the extract.
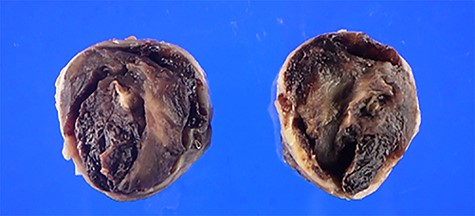
Cross-section of the removed aneurysm. An arrow indicates the coil.
DISCUSSION
Aneurysms are bulging aneurysms caused by degeneration of the arterial wall. Abdominal and thoracic aortic aneurysms are known. Although there are no clinical symptoms initially, their rupture may be a cause of death in middle-aged and elderly people. A true aneurysm is the enlargement of the wall structure of the artery without traumatic injury in which the blood is retained inside the circulatory system [1–5]. It involves all three layers of the arterial wall (intima, media and adventitia). Most true aneurysms are associated with atherosclerosis [6]. In contrast, a false aneurysm arises from partial injuries of vessel wall. A rupture of the arterial walls leads to overflow of blood into the surrounding tissue in cases of false aneurysm. Therefore, a false aneurysm is described as an extravascular hematoma that communicates with the intravascular space via a rupture of the vessel wall [1, 7–9]. The report of true aneurysms is uncommon, especially true aneurysms of the facial artery that branches from the external carotid artery are extremely rare. The surgical management of true aneurysms of the facial artery is not been widely acknowledged.
To date, only five cases of true aneurysm have been reported [1–5]. In the previously reported cases, the sizes of the reported aneurysms ranged from 1.5 to 5 cm, the median age of the patients was 68 years old, and three of the five cases [2–4] had no history of cardiovascular disease. The prevalence of true aneurysms in older patients may support reports of an association with atherosclerosis [6]. The male:female ratio for the occurrence of true aneurysms was 4:1, indicating a higher incidence in males [1–5]. Treatment of aneurysms is known to involve ligation, resection and embolization. Four previously reported cases [1–3, 5] selected excision as a treatment strategy and embolization was performed in the fifth case [4]. Therefore, this is the first case of surgical excision of the true aneurysm after internal trapping. The advantage of this treatment strategy is that it prevents the risk of bleeding during surgery and restores cosmetic appearance; further the diagnosis can be confirmed by resection.
In this case, it was difficult to determine whether it was an aneurysm or a submandibular gland tumor with pseudoaneurysm only by imaging. This may be because the layers of the arterial wall of the true organized aneurysm and the capsule seen in a submandibular tumor (like pleomorphic adenoma) appear similar on imaging and encapsulated masses in the neck are often considered submandibular tumors epidemiologically. Therefore, it was considered desirable to perform extirpation to make a definitive diagnosis in this case.
In conclusion, we show that there is a need to suspect a vascular lesion in the head and neck region in case of swelling and that surgical excision after internal trapping is a suitable treatment for true aneurysms.
ACKNOWLEDGMENT
The authors are grateful to neurosurgeons Dr Yoshimura and Dr Nakanishi for helpful discussions and contributions.
CONFLICT OF INTEREST
None declared.
FUNDING
None.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}