





Abstract
Endometriosis of the abdominal wall is a rare entity, the etiopathogenesis remains unclear. It most often occurs after gynecological or obstetric surgery. We report the case of a patient with a dual localization of endometriosis in the abdominal wall, the diagnosis was made by abdominal CT scan. The treatment was surgical. The pathology study confirmed the diagnosis of parietal endometriosis. The postoperative course was uneventful with a favorable outcome for 2 years without recurrence. Through our case, we will discuss the characteristics of this entity in order to understand the interest of an early diagnosis and management to deduce possible means of prevention during each gynecological or obstetric surgery.
INTRODUCTION
Endometriosis corresponds to the presence of functional endometrial tissue in an ectopic situation outside the uterine cavity. The most common locations are pelvic [1]. The abdominal wall location is rare [2]. The rectus muscles location is very exceptional [1]. Few case reports have been published to date since its first description in 1984 by Amato and Levitt [3]. The etiopathogenesis remains imprecise [4]. The originality of this work is the double localizations of extrapelvic endometriosis. The aims of this work are to discuss through our observation the clinical characteristics, the treatment and the evolution of these lesions from a review of the literature to deduce possible means of prevention.
OBSERVATION
A 31-year-old women, with no history, presents 4 years after a cesarean (incision of Pfannenstiel), two masses one at the level of the left iliac fossa above cesarean scar, and the second one in the lower left rectus muscle gradually increasing in volume, and painful at the time of menstruation. The abdomen examination found an irregular wall tumor of 2 cm, firm, painful, at the level of the left iliac fossa and another of 5 cm in the rectus muscle without cutaneous erythema. An abdominal CT revealed a subcutaneous masse of 2.1 × 1.7 cm in the left iliac fossa and another mass involving the rectus muscle and fascia without traversing the peritoneum (Fig. 1). Elective surgery was performed. During surgery, the two masses were observed, the excision was performed including a 10-mm safety area of each them (Fig. 2). Hemostasis was achieved by ligation of the vascular pedicle entering at the periphery of the mass. Due to a significant defect in the aponeurosis, a polypropylene mesh was used (Fig. 3). Pathology examination confirmed the presence of foci of cystic and hemorrhagic endometriosis (Fig. 4). The postoperative course was uneventful. The patient had a favorable outcome for 2 years without recurrence.
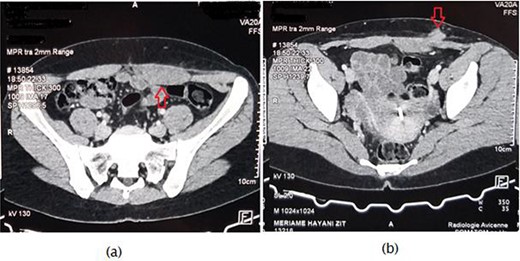
Axial computed tomography scan revealing (a) nodular hypertrophy of the lower left rectus abdominus, (b) mass of 2.1 × 1.7 cm in the left iliac fossa in touch with the rectus muscle.
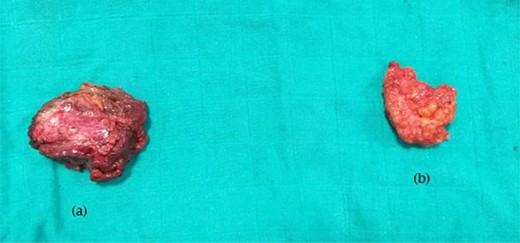
(a) surgical specimen of rectus abdominis endometrioma, (b) surgical specimen of subcutaneous left iliac fossa endometrioma.
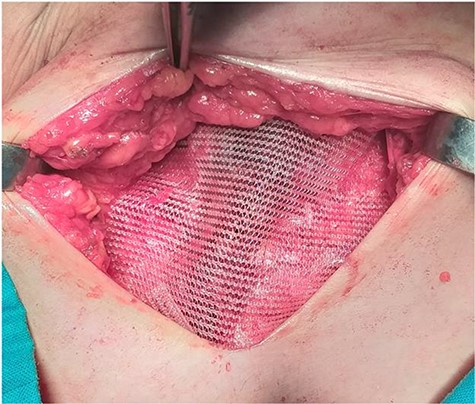
The use of a polypropylene mesh after R0 resection with significant defect in the aponeurosis.
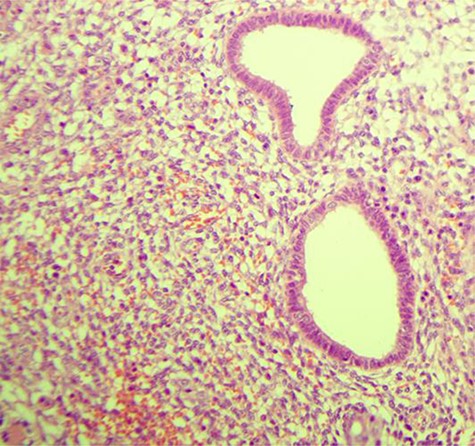
Endometrial glands surrounded by stroma (HE, ×200).
DISCUSSION
Endometriosis of the abdominal wall is a rare entity. It represents 0.03–2% of extragenital endometriosis [5]. Due to its asymptomatic nature, the exact prevalence is unknown [6]. The incidence after cesarean section is 0.03–0.4% [7]. The endometriosis etiopathogenesis can be explained by three theories [8]: the transplant theory is based on the migration of endometrial fragments by the tubal reflux; the theory of coelomic metaplasia evokes the possibility of transformation of epithelium coelomic cells in endometriotic metaplasia—the exact stimulus triggering this transformation is unknown; and finally, the metastatic theory evokes the possibility hematogenous or lymphatic dissemination.
Anterior abdominal wall endometriosis is classically manifested like our case with a localized, tense and painful tumor, increased at menstrual period, on or near a scar of gynecological surgery [9]. The interval time between operation and presentation varied. In our case it was 4 year, in the literature it is between 3 months and 10 years [7]. There are many differential diagnoses such as eventration, hematoma, granuloma, abscess, lymphadenopathy, lipoma, neurofibroma, sarcoma and desmoid tumor [1]. Once the parietal endometriosis is suspected, Sonography and Doppler could contribute to preoperative diagnosis, they can show an image with fluid or mixed content, hypoechoic or hyperechoic depending on the phase of the menstrual cycle [4]. Anecdotal studies have mentioned the use of computed tomography (CT) like our case and magnetic resonance imaging (MRI) in making a diagnosis. CT scan usually shows a solid, well-circumscribed mass [7]. MRI can be more helpful when the lesion is small because of its high spatial resolution. It can show a T1 hypersignal which may be in favor of intralesional bleeding. The presence of a T2 hyposignal wall encircling the lesion is fairly characteristic of endometriosis. MRI can also be used to specify the depth extension of the endometrioma. Fat saturation sequences eliminate the dermoid cyst. Finally, the sensitivity and specificity of MRI for the diagnosis of endometrioma are, respectively, 90 and 98% [10]. The percutaneous biopsy has been reported by some authors but should be banned due to the risk of dissemination along the path of the puncture [4].
Medical treatment with LH-RH agonists or Progestogens has been tried and although it allows to decrease symptoms, it does not allow the healing of lesions which recur quickly; this can be explained by the low quantity of hormone receptors compared with the size of tumor mass [1].
Medical treatment can be designed as an induction treatment for big masses, aimed at reducing the volume of the endometrioma and the parietal defect resulting from its excision. Moreover, the exceptional endometrioid carcinoma, reported for extragenital localizations, constitutes an additional argument in favor of surgical excision [6].
The treatment of choice for endometriosis of the rectus abdominis muscle is a wide local excision of the lesion with negative margins. The surgical excision should include 5–10 mm of the surrounding healthy tissue as surgical margin and care must be taken not to rupture the mass to avoid reimplantation of microscopic remnants of endometrial tissue [7]. The parietal reconstruction after excision requires sometimes the setting up of a parietal mesh when the musculo-fascial banks closure is impossible. The Poly-propylene mesh is particularly useful to make up for the loss of substance induced by parietal excision [1].The same procedure was followed in our case.
Prevention in case of laparotomy is based on abundant washing of the abdominal cavity and scar at the end of the intervention as well as the change of gloves for the time of parietal closure, while in laparoscopy, the extraction of the specimen should be in a protective bag and abundant washing of the pelvic cavity should be systematic. Thus, these measures are part of good surgical practice although their benefit has never been demonstrated [5].
CONCLUSION
The anterior abdominal wall endometriosis is a rare entity. The diagnosis should be suspected in localized, painful tumor that increased at menstrual period happening after a gynecological surgery. To confirm this hypothesis, MRI is the most adapted. The medical treatment can be used to reduce the size of big endometrioma, however surgery is the definitive treatment and should be carcinological.
Conflicts of interest
None declared.
FUNDING
None.
Author contributions
All the authors testified to the care of the patient and the writing of the manuscript. The authors have read and approved the final version of the manuscript.

{kind=link}
{kind=link}
{kind=link}
{kind=link}