





Abstract
This article presents a rare case report of an ectopic third molar tooth located in the medial wall of maxillary sinus in a young male manifesting as recurrent sinusitis along with upper jaw pain and postnasal discharge diagnosed with an ectopic tooth and bilateral dentigerous cysts. This article aims to discuss this rare presentation of an ectopic tooth as a cause of recurrent maxillary sinusitis and the endonasal endoscopic management of the case.
INTRODUCTION
Tooth development occurs by means of a complicated multistep interaction between the oral epithelium and the underlying mesenchymal tissue. Abnormal tissue interaction during this process can result in ectopic tooth development [1]. Ectopic tooth eruption may result owing to one of three processes: pathological process, such as tumor or cyst, developmental disturbance, or iatrogenic activity [1, 2]. Although it is common to occur within the dentate region, an ectopic eruption of a tooth in nondentate areas is a rare entity [3].
Ectopic teeth generally remain asymptomatic for several years before being noticed incidentally on routine radiographic examination. However, when they erupt in the maxillary sinus, this can cause local sinonasal symptoms [2, 4]. Ectopic teeth obstructing the sinus ostium are rarely reported in the literature [5].
The treatment of such pathological condition in the maxillary sinus includes surgical removal whenever possible because if left untreated, it has the tendency to form a cyst or tumor and may also cause perforation of the orbital floor and obliteration of the nasal cavity [4].
In this article, we report a case of recurrent maxillary sinusitis associated with the presence of an ectopic third molar in the maxillary sinus obstructing the sinus ostium.
CASE REPORT
A young male was referred to the Department of ENT at our hospital, with the complaint of facial pain over the upper jaw area along with postnasal discharge. This complaint has developed over a period of 6 months prior to his presentation. The patient gave a history of recurrent sinusitis but had no systemic illness and gave no history of trauma.
Clinical examination was unremarkable except for a septal spure to the left side for which paranasal sinus computed tomography (CT) scan was done (Fig. 1).
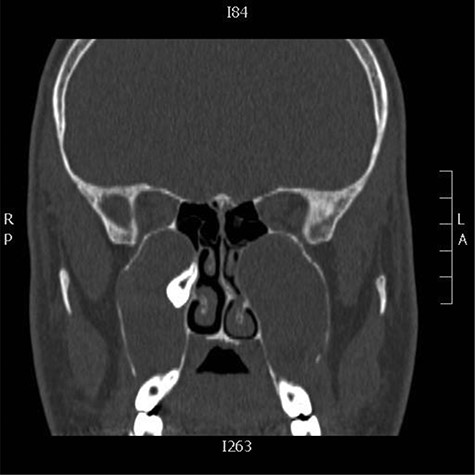
Coronal CT images showing bilateral cystic lesions in the maxillary antra with expansion and remodeling of the roof, lateral and medial walls, the right cystic lesion displaces ectopic tooth superiorly and medially in the region of the expanded remodeled ostiomeatal complex
Intraoperative, the right middle meatus was full of frank pus (Fig. 2) which was drained. Endoscopic middle meatus antrostomies was performed and a bilateral big cystic masses completely filling both maxillary sinus were visualized along with a tooth impacted in the medial wall of the right maxillary sinus obstructing the natural drainage. The diagnosis of bilateral dentigerous cysts with ectopic teeth was made on clinical and radiographic findings.
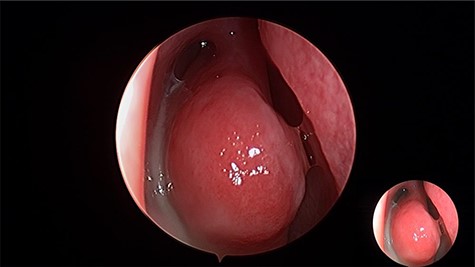
Intraoperative endoscopic view of frank pus draining the right maxillary sinus
Endoscopic removal of the ectopic molar tooth (Fig. 3) along with dissection and removal of both cysts. With the help of different angled endoscopes and forceps.
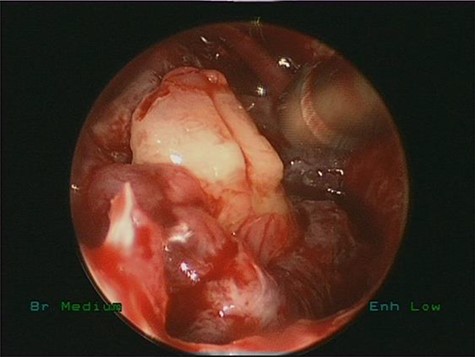
Intraoperative endoscopic view of ectopic tooth and the cyst, the patient’s symptoms were resolved completely postoperatively and remained symptoms free for 4 years follow-up
DISCUSSION
The mandible is the most frequent anatomic location of ectopic teeth. The most commonly associated teeth are the incisors, canines and premolars [8]. Eruption of ectopic teeth into nondentate regions is rarely reported in the literature [3, 6]. Although there have been reports of teeth in various regions of jaws such as mandibular condyle, coronoid process, nasal septum, palate and rarely, as in our case, maxillary sinus [6]. Ectopic teeth obstructing the sinus ostium is a rare entity. It causes morbidities sometimes differentiated with the most common causes of sinus ostium obstruction like foreign bodies, sinonasal tumors of any origin, sinonasal polyposis and others [8].
The etiology of developing an ectopic tooth is not yet exactly understood. However, these teeth can result from trauma, infection, developmental anomalies such as cleft palate, pathologic conditions such as dentigerous cyst, iatrogenic or idiopathic factors [1].
Ectopic teeth mostly have no symptoms. Nevertheless, when they present in the maxillary sinus this can cause several symptoms, most frequently a facial pain, facial swelling, headache, purulent discharge, recurrent sinusitis, epistaxis and nasolacrimal obstruction [1–3, 7]. These teeth may also lead to the formation of cysts and other pathologies in the area [9]. In our case, the chief complaint was facial pain involving the area of the upper jaw and recurrent postnasal discharge.
Radiological examination can easily detect and diagnose ectopic teeth due to their radiopaque image, especially when these teeth are localized to the maxillary sinus [6, 7]. Panoramic radiograph, radiographs of the maxillary sinus such as Water’s graphy, and especially CT are useful for the localization of the ectopic teeth. CT imaging is gold standard in such conditions to determine the definite localization [7]. It allows for a larger area detailing, thus optimizing surgical planning, once it is possible to visualize the tooth structure morphology, and root inclination and position in relation to the underlying structures. Thus, it is possible to predict eventual transoperative intercurrences, postoperative complications and prognosis [1, 10]. In our case, the CT scan allowed the observation of the exact location of ectopic tooth located at the medial wall of maxillary sinus causing sinus obstruction and recurrent sinusitis.
Differential diagnosis of ectopic teeth in the maxillary sinus includes (i) infections such as tuberculosis, syphilis or fungal infections with calcification, (ii) benign lesions such as hemangioma, osteoma, calcified polyp and enchondroma, (iii) foreign bodies (rhinoliths) and (iv) malignant lesions such as osteosarcoma, chondrosarcoma must be regarded [7].
The standard treatment in symptomatic cases is surgical removal. Due to the difficulty of reaching the lateral, anterior and inferior walls of the maxillary sinus, a combined approach of endoscopic and Caldwell–Luc procedure was the commonly used approach. However, in our case, the endonasal endoscopic removal of the tooth was achieved with the help of different angled scopes and forceps with uneventful recovery.
CONCLUSION
This article presents a rare case of an ectopic third molar tooth located in the medial wall of maxillary sinus in a young male manifesting as recurrent maxillary sinusitis along with upper jaw pain and postnasal discharge. CT scan confirmed the diagnosis and location of the ectopic tooth obstructing the maxillary sinus.
The endonasal endoscopic approach is a direct minimally invasive procedure to such case with no morbidities and avoiding the external surgical approach.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
None.

{kind=link}
{kind=link}
{kind=link}