





Abstract
We present a case of dialysis associated steal syndrome in a hemodialysis patient with left radiocephalic arteriovenous fistula that caused him severe rest pain. Angiography showed retrograde flow from the ulnar artery to the distal radial artery through a hypertrophied palmar arch. The problem was solved by surgical ligation of the distal radial artery leading to complete relief of patient symptoms without any notable complications.
INTRODUCTION
One of the major complications of arteriovenous fistula (AVF) creation is the development of dialysis associated steal syndrome (DASS), resulting in significant hand ischemia in some patients. Severe symptomatic DASS more commonly occurs in patients with brachial artery origin, diabetes mellitus (DM) and female gender. Other risk factors include previous ipsilateral AVF, peripheral atherosclerosis and age [1]. The incidence of symptomatic DASS is much less common in AVF performed in the forearm compared with those in the arm ranging from 0.25 to 1.8% [2]. The rationale of creating a more distal upper limb fistula is to preserve blood supply to the hand by preserving at least one of the forearm vessels. This was highlighted in a large cohort of high-risk patients for developing DASS by performing the AVF anastomosis on proximal radial or ulnar artery resulting in very low incidence (2.8%) of DASS [3].
Although the ligation of the AVF usually gives ultimate relief of symptoms, the aim of the management of patients with DASS is always to treat its manifestations without losing the access, especially in patients with limited access options. Access banding is a widely used solution, but it has high risk of thrombosis and re-intervention. Most of the other treatment options for DASS such as distal revascularization with interval ligation (DRIL), proximalization of the arterial inflow and revision using distal inflow (RUDI) are mainly used for arm, but not distal forearm AVFs [4].
In this article, we present a case of distal radial artery ligation for relief of symptoms of DASS in a patient with radiocephalic (RC) AVF that was stealing the blood flow from the ulnar artery through the palmar arch.
CASE REPORT
A 71-year-old male patient, with end-stage renal disease secondary to DM and hypertension associated with the history of hyperlipidemia, peripheral vascular disease and ischemic heart disease, was reviewed in kidney dialysis unit for severe pain in the left hand since 1 month. This pain was aggravated during dialysis, but it was also present at rest. The patient was receiving hemodialysis (HD) three times a week through a functioning left RC AVF, which was created 4 years ago.
Physical examination showed a well-developed left RC AVF with a palpable thrill and two aneurysmal dilatations of the cephalic vein at sites of needling for HD. His radial pulse was not palpable distal to the AVF, but it had monophasic Doppler signals. It was also noticed that applying pressure over the course of radial artery distal to the AVF anastomosis caused transient symptomatic relief with reactive hyperemia of the hand. The patient did not have thenar muscle wasting and Tinel’s test was negative for carpal tunnel syndrome.
Digital brachial index was 0.5 and TcPO2 was 28 mm Hg. Duplex scanning showed retrograde flow in the radial artery distal to the AVF anastomosis and the amount of blood flow through the AVF was 700 mL/min.
Angiography was done through a brachial artery access, which showed complete absence of antegrade flow in the radial artery distal to the AVF anastomosis with filling of this segment of the radial artery by retrograde flow from the ulnar artery (Fig. 1), whereas the whole flow in radial artery was directed to the AVF (Fig. 2) with a well-developed palmar arch (Fig. 3).
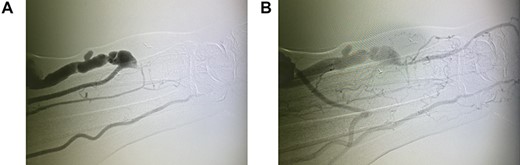
Digital subtraction angiography (DSA) through brachial artery (A) early image showing filling of the ulnar artery and all blood in radial artery is going to the RC AVF (B) late image showing the filling of the radial artery distal to the AVF anastomosis from the ulnar artery by retrograde flow through the palmar arch.
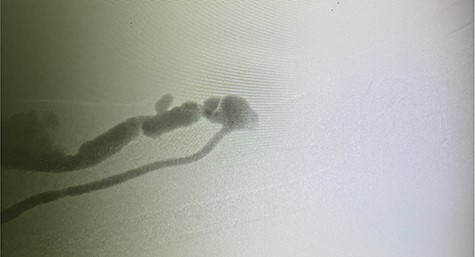
Selective radial artery DSA with shunting of all the blood in radial artery to RC AVF with complete absence of antegrade flow in radial artery beyond the anastomosis.
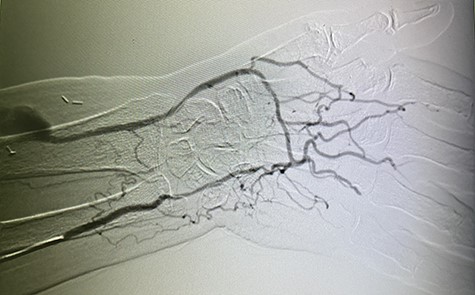
Selective ulnar artery DSA showing well-developed palmar arch with retrograde flow in the distal radial artery to supply the RC AVF.
The decision was made to ligate the radial artery distal to AVF anastomosis. All risks and benefits were explained to the patient and informed consent was obtained.
The ligation of the distal radial artery was performed under local anesthesia through a 3-cm incision, and a 2/0 silk suture (Ethicon Inc., Mersilk, XCW213, P31) was used to tie off the artery. The patient was discharged home on the next day without any complications after performing dialysis through the AVF. There was also significant decrease in the pain, previously experienced by the patient on the same day of operation and near total disappearance of pain after 2 weeks during follow-up in the outpatient clinic. Furthermore, his fistula is patent and still functioning to date after 6 months from the operation.
DISCUSSION
One of the hemodynamic changes after AVF creation is the retrograde flow in the distal radial artery, which occurs in 70% of RC AVFs, but it is rarely a cause of ischemia [5]. It is noted that the onset of DASS in RC AVF occurs after a long time of AVF creation; 4 years in our case and 5.5–11 years in other case reports [5, 6]. Hemodynamically, the blood tends to go to the lower resistance circulation, which is cephalic vein in RC AVF, instead of going distally to the higher resistance circulation in the digits. The hypothesis behind late onset of DASS in RC AVF is that initially the flow reversal is not significant enough to cause ischemic manifestations at the time of fistula creation. However, with time, the palmar arch will become hypertrophic to cope with increasing retrograde flow and this will significantly decrease the perfusion of the digits. More dedicated studies are needed to prove this hypothesis.
We performed conventional angiography to detect any arterial stenosis or occlusion and to exclude DASS. Based on the mentioned findings, we considered the interruption of flow in the distal radial artery to help hand perfusion through the ulnar artery and prevent its shunting to the RC AVF. The interruption of the distal radial artery flow can be performed either by open surgical ligation or endovascular coiling and embolization [7]. We decided to do surgical ligation, as it is an easy procedure, cost-effective, done through a mini-incision and does not carry any risks related to distal embolization of the coils.
Banding of AVF is an option to solve the problem. However, it has a variable success rate and high risk of early thrombosis [4]. DRIL is an effective technique for the treatment of DASS with overall success of 81% during a mean follow up of 22.2 months [8]. RUDI is another effective solution for DASS showing overall success rate of 82.0% over 12 months in a systematic review involving 11 studies [9]. However, both DRIL and RUDI are usually performed in the arm and rarely in distal forearm AVFs.
CONCLUSION
Distal radial artery ligation is a safe and viable option for both symptomatic relief of DASS, and the salvage of RC AVF provided there is adequate ulnar artery perfusion of the hand, especially when the retrograde flow in radial artery from the ulnar artery is proven by angiography.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}