





Abstract
Colonic lipomas are the most widespread non-epithelial tumours of the large bowel. They often present with absent, non-specific or intermittent symptoms. Intussusception is the most common complication that may occur as a result of such a lesion. We present the case of a young female patient with a history of intermittent abdominal pain associated with nausea. She presented to the emergency department with subacute large bowel obstruction. A diagnosis of colo-colic intussusception due to a large descending colonic lipoma was confirmed on CT scan. The patient underwent a laparoscopic assisted submucosal excision of the lipoma. We discuss this unique operative technique as well as preoperative investigations and histopathology findings. Although successful endoscopic excision of lipomas has been reported, segmental resection of the colon is most commonly practiced. To the best of our knowledge, this is the first report of laparoscopic assisted submucosal excision of an intussuscepting colonic lipoma.
INTRODUCTION
Though lipomas can be found throughout the digestive system, colonic lipomas are the most common (64%). They are the most frequent non-epithelial tumours of the colon [1,2]. Lipomas of the colon are seen more often in women than in men and ~90% of colonic lipomas are in the submucosal space1.
Symptomatic colonic lipomas are a rare entity in adults. Lipomas <4 cm are very unlikely to cause significant symptoms [3]. Intussusception is the commonest complication of submucosal lipomas and often presents with absent, non-specific or intermittent symptoms, hence the diagnosis is challenging. In adults, 5% of cases of bowel obstruction are caused by intussusception [4].

Radiological findings, (A)AXR, gaseous distention of the colon as far as mid-descending colon (B) CT, large bowel obstruction with transient point in the mid-descending colon secondary to large bowel intussusception.

Submucosal Lipoma located in the mid-descending colon.
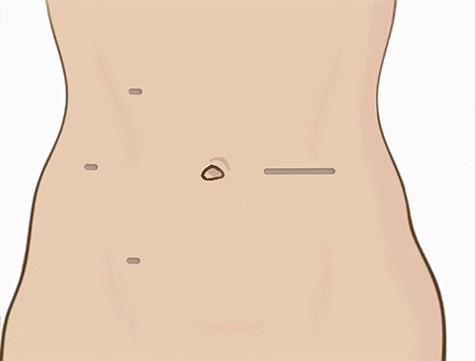
Port sites and extraction incision.
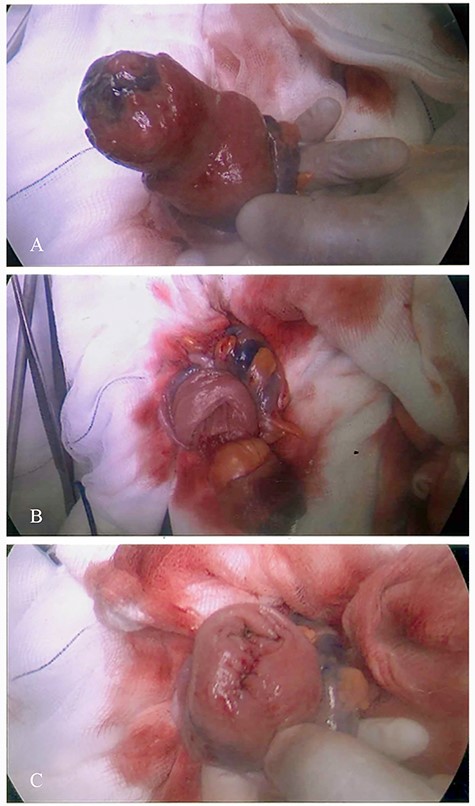
Surgical procedure demonstrating submucosal excision; (A): lipoma delivered through a colotomy, (B): submucosal excision and (C): closure of the mucosal defect.
In non-emergency situations, most patients undergo computed tomography scan as well as endoscopic evaluation of the colon prior to any surgical intervention. Although successful endoscopic excision of lipomas has been reported [5] in the non-acute setting, segmental resection of the colon is most commonly practiced in cases of intussusception and obstruction.
CASE REPORT
A 40-year-old female presented to the emergency department with worsening symptoms of colicky abdominal pain, distention, vomiting and haematochezia. She had been suffering with these symptoms intermittently for about 2 months. Her pain was mainly located in the left iliac fossa and she had experienced episodes of loose stools mixed with dark red blood. Four days prior to her admission, she had had a colonoscopy in a different centre to investigate her ongoing symptoms.
She did not have any significant co-morbidity but her past medical history included a diagnosis of a right ovarian cyst and a previous uterine polypectomy.
On examination she was haemodynamically stable, her abdomen was soft but distended with generalized tenderness, mainly in the left iliac fossa. Digital rectal examination revealed an empty collapsed rectum.
The laboratory examination on admission demonstrated no anaemia and unremarkable renal function; specifically her white cell count was 10.5 (109/L), Hb 127 (g/L), Na 138 (mmol/L), K 4.8 (mmol/L), Urea 2.1(mmol/L) and creatinine 71 (μmol/L).
Erect chest and abdominal X-ray was performed which showed gaseous distension of the colon as far as the mid-descending colon with very little gas distal to this (Fig. 1A). Consequently a computed tomography (CT) scan of her abdomen and pelvis was obtained which confirmed the plain X-ray findings and showed gaseous distension of the transverse colon with a transition point in the mid-descending colon where a colo-colic intussusception was demonstrated due to a large descending colon lipoma. The distal colon beyond the intussusception was completely collapsed (Fig. 1B).
The patient’s obstructive symptoms resolved following administration of adequate analgesia and anti-spasmodic medication (Hyoscine). As she remained stable with no biochemical finding or radiologic features suggestive of ischemia or impending perforation, an urgent flexible sigmoidoscopy was arranged which showed a large mid-descending submucosal colonic mass with a smooth surface and mucosal ulceration, confirming the radiological impression of a submucosal lipoma (Fig. 2).
Rather than subject the patient to a left hemicolectomy, we decided on a minimally invasive laparoscopy assisted transcolonic resection of the lipoma. Pneumoperitoneum was achieved following the insertion of a 5 mm Ethicon Excel port in the right flank. Following carbon dioxide insufflation, other ports inserted as shown on Fig. 3. After adequate mobilization of the sigmoid and descending colon, the intussuscepted segment of the descending colon was identified. A small muscle-splitting incision was made at the level of the umbilicus in the left side of the abdomen (Fig. 3) and the pathological segment of colon was pulled to the surface through a small Alexis wound protector. The lipoma was palpated within the exteriorised bowel and a colotomy performed through the taenia on the opposite wall at the level of the lipoma. A mucosal incision was made around the base of the lipoma and the entire lipoma was shelled out and removed through the colotomy (Fig. 4). Following closure of the mucosal defect with 3/0 Vicryl, the colotomy was closed using interrupted sutures of 3/0 monofilament synthetic absorbable suture (PDS® II (polydioxanone) Suture, Ethicon).
Post-operatively, the patient made an uneventful recovery and was discharged on Day 4. The histopathology of the specimen confirmed a benign submucosal lipoma (Fig. 5). The patient was followed up 6 weeks later, was totally asymptomatic and was discharged from surgical care.
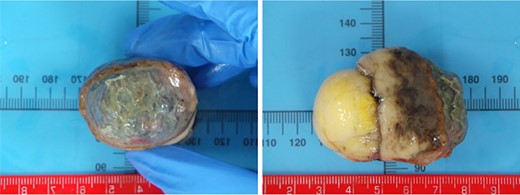
Pathology: visual representation of specimen.
DISCUSSION
Colonic lipomas are rare benign lesions of gastrointestinal tract with a worldwide frequency of 0.035–4.4% [6]. They are most commonly located in the ascending colon and cecum. However, intussusception due to colonic lipoma has been frequently reported in the transverse and the descending colon [7].
CT scan is a valuable diagnostic aid to determine the underlying pathology of the bowel obstruction secondary to intussusception. Gastrointestinal lipomas are typically a homogeneous mass with Hounsfield units between −80 and −120 [8].
Surgical resection should be considered for large or symptomatic lipomas that are sessile, have limited peduncles, or are not suitable for endoscopic resection. The usual surgical techniques described in literature are hemicolectomy and segmental resections [9,10]. To the best of our knowledge, this is the first report of laparoscopic assisted submucosal excision of an intussuscepting colonic lipoma through a colotomy. We believe this technique should be strongly considered when the pre-operative diagnosis of a lipoma is confirmed in order to limit perioperative and long-term morbidity.
AUTHOR’S CONTRIBUTION
F.E. wrote the paper and operated on the patient. E.M. collected the data for the case report and wrote the paper. V.V. revised the manuscript and operated on the patient.
ACKNOWLEDGEMENTS
The authors gratefully acknowledge Rebecca Parrott, Clinical Outreach Librarian at The Princess Alexandra Hospital NHS Trust, for her assistance with literature search.
CONFLICT OF INTEREST STATEMENT
None declared.
COMPLIANCE WITH ETHICAL STANDARDS
Authors confirmed that informed patient consent was obtained for publication of the case details.
Funding
None.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}