





Abstract
Metastatic breast carcinoma is a relatively common clinical entity. However, the prognosis of oligometastatic and polygometastatic disease differs considerably pertaining to five-year survival. Metastatic breast carcinoma to the sternum has been described as early as 1988. We describe two cases in our institution who presented with solitary sternal metastases with a previous history of treated breast cancer. In both cases, there had been a history of previous left breast cancer treated aggressively with surgical resection and adjuvant oncological therapy and maintenance hormonal therapy. Partial sternectomy or total sternectomy for solitary metastatic sternal deposits is well established with relatively low morbidity and mortality and improvement in quality of life and possible improvement in long-term survival. Furthermore, reconstructive options are inherently dependent on extent of resection performed. These techniques can incorporate the use of sternal plates in order to approximate defects and reinforce the sternum in the setting of partial sternectomy.
INTRODUCTION
Metastatic breast carcinoma is a relatively common clinical entity with 20–30% of patients with early-stage disease developing metastases and 3–6% with de novo Stage IV disease at time of initial diagnosis [1]. However, the prognosis of oligometastatic and polygometastatic disease differs considerably pertaining to five-year survival. Furthermore, the survival and procedure-related morbidity and mortality data for any surgical resection are largely based on retrospective data analysis of multiple cases performed at a single-centre or multicentre studies rather than from any randomized controlled trial. Therefore, there is considerable debate and contention about the efficacy of metastasectomy and its widespread application in clinical practise. Utilizing equivalent strategy and principles of pulmonary metastasectomy, any surgery for metastatic disease is founded on the core principles outlined by Thomford et al. [2] in 1965. These include control or eradication of primary site of cancer and exclusion of local recurrence, relative disease-free interval with a longer disease-free interval indicating a better prognosis, surgically resectable disease and availability of adjuvant oncological therapy. There have been discussions regarding the cytoreductive aspect of metastasectomy, but this is well established due to the concept of micrometastatic disease in cases where complete resection is not possible and it is generally accepted that incomplete metastasectomy probably offers no significant advantages but potentially carries a considerable morbidity and mortality risk. Metastatic breast carcinoma to the sternum has been described as early as 1988 [3]. Furthermore, one of the earliest case series in 1988 described a series of nine patients with solitary sternal metastasis who underwent partial or total sternectomy. In this study, patients with solitary metastatic sternal deposits without evidence of other regional spread favoured considerably compared with those with sternal deposit oligometastatic disease that had spread to other sites. The authors of the study concluded that resection of solitary sternal metastasis should be advocated and that in addition to improving quality of life, survival may also be improved [3]. Similarly, the efficacy of partial or total sternectomy in patients with solitary metastatic sternal spread has been demonstrated subsequently [4]. There have been numerous cases discussing sternal resection and reconstruction often with the use of methyl methacrylate and acrylic cemented prostheses [5–6], Marlex mesh and muscle flaps to cover defects [4]. We describe two cases in our institution who presented with solitary sternal metastases with a previous history of treated breast cancer.
CASE REPORT
The first case at our institution was a 39-year-old woman who had a history of left breast carcinoma treated with left mastectomy, axillary node clearance and immediate reconstruction under the care of the breast team 3 years prior to presentation. She had no significant co-morbidities. Her past surgical history consisted of the aforementioned oncological operation, appendicectomy and cholecystectomy. She had completed adjuvant oncological therapy in the form of chemoradiotherapy and maintenance hormonal therapy. Her post-operative histology was consistent with a fully excised left breast ductal carcinoma and spread to three out of nine lymph nodes. Due to positive oestrogen receptor-2 status, she had been placed on hormonal therapy. She re-presented with chest wall and sternal pain and subsequent computer tomography (CT) imaging demonstrated a suspicious looking lytic lesion in the mid-sternum (Fig. 1). She underwent a biopsy of this lesion, which confirmed the diagnosis. She had been taking opioid medication for the pain. She was seen in clinic and counselled for partial sternectomy and reconstruction. She underwent partial sternectomy and underwent reconstruction with vertical and horizontal Synthes® plates. Her post-operative recovery was unremarkable. Post-operative histology was consistent with metastatic breast carcinoma completely excised. The recovery was uncomplicated and the patient was seen in clinic with a satisfactory chest radiograph demonstrating the sternal Synthes® plates (Fig. 2).
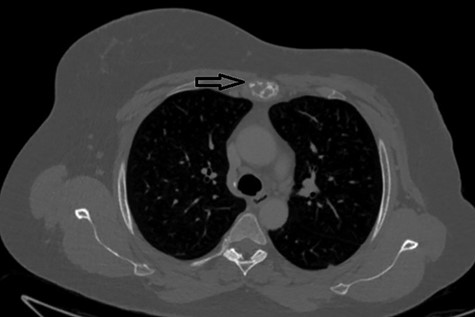
Lytic mid-sternal lesion on CT (arrow).
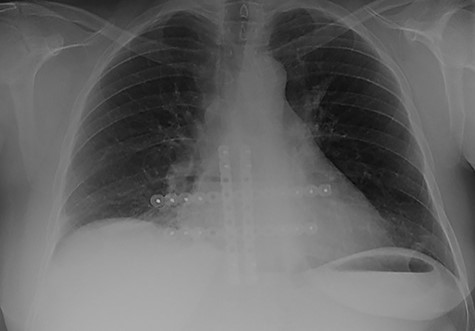
Follow-up chest radiograph demonstrating the fixation plates.
The second case at our institution was a 52-year-old woman with a history of left breast carcinoma treated for which she had undergone left wide local excision and sentinel node biopsy. Due to uncertainty regarding margins, she required a re-resection of her left breast tissue. She completed adjuvant radiotherapy and received maintenance hormonal therapy. She presented 8 months following her radiotherapy with sternal pain and positron emission tomography–computed tomography (PET–CT) imaging demonstrated localized uptake within the sternum (Fig. 3). Biopsy demonstrated proven recurrence of metastatic breast cancer. She was seen in clinic and counselled for partial sternectomy and reconstruction. She underwent partial sternectomy and underwent reconstruction with Synthes® plates. Her post-operative recovery was unremarkable. Post-operative histology was consistent with metastatic breast carcinoma, which was completely excised. The patient made an uncomplicated recovery and was seen in the outpatient clinic with a satisfactory post-operative chest radiograph (Fig. 4).
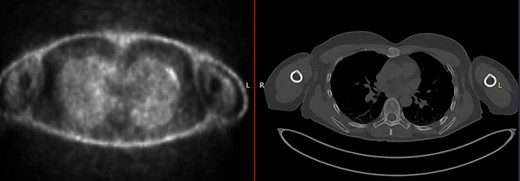
CT–PET demonstrating increased metabolic activity within the sternal lesion.

Follow-up chest radiograph of second patient.
DISCUSSION
Partial or total sternectomy for solitary metastatic sternal deposits is well established with relatively low morbidity, mortality and improvement in quality of life and long-term survival [7]. Interestingly, the aspect of chest wall or sternal pain is one aspect that considerably improves following sternal metastasectomy. Chest wall resection and reconstruction for metastatic breast cancer has been demonstrated to be effective in certain cohort of breast cancer patients with low mortality and morbidity [8]. In addition to surgery, cryoablation has also been purported as an effective alternative to radial surgical resection to achieve loco-regional control [9]. Upon review of the relevant literature, the application of surgery seems universal in that localized disease and recurrence in the sternum should be resected [4]. However, the type of resection partial or total sternectomy is dependent on the size of the tumour and the principle of achieving complete excision. Reconstructive options have been performed via a multitude of methods and involve using cemented prostheses, Marlex mesh and muscle flaps [4] and in some cases of total sternectomy, customized 3D-printed titanium prostheses [10]. Our experience involves partial sternectomy for localized sternal recurrence and reconstruction of the defect using Synthes® plates to reinforce and stabilize the sternum. In summary, metastasectomy, either as partial or total sternectomy, should be performed for localized sternal recurrence for metastatic breast cancer as long as the core principles of metastasectomy are observed. Furthermore, reconstructive options are inherently dependent on extent of resection performed. These techniques can incorporate the use of sternal plates in order to approximate defects and reinforce the sternum in the setting of partial sternectomy.
Conflict of interest statement
None declared.
FUNDING
None.

{kind=link}
{kind=link}
{kind=link}
{kind=link}