





Abstract
Among synchronous colorectal cancers (SCRCs) reported previously, the incidence of quadruple advanced SCRCs is very rare. We present the case who underwent laparoscopic two-segment resection of the colon requiring two anastomoses that was performed for quadruple advanced cancers, and four tumors were curatively removed. There were no signs of recurrence at 64 months after surgery. Laparoscopic surgery provided less invasiveness even for quadruple advanced SCRCs in terms of early recovery with an acceptable long-term outcome.
INTRODUCTION
Synchronous colorectal cancers (SCRCs) are characterized by the simultaneous occurrence of multiple primary tumors in the same patient. Synchronous malignancies most commonly occur in the colon among other organs [1–3]. The occurrence of advanced SCRCs is rare and may be identified at any location within the large intestine [2]. The prevalence of SCRCs is reported to range from 1.1 to 8.1% [3]. Among these, however, the incidence of quadruple advanced SCRCs is extremely rare, accounting for 0.16% of all SCRCs [4]. Surgical resection is considered the standard treatment for SCRCs [5]. As a surgical approach, laparoscopic surgery has significant advantages in terms of short-term outcomes including early recovery and no disadvantageous long-term outcomes. According to recent reports, laparoscopic surgery has been used in SCRCs [6], but these reports noted that controversy remains concerning operative procedures for multiple segmental resections and for total or subtotal colectomy. We report the case who presented with quadruple synchronous advanced cancers arising from the colon, which were successfully treated with laparoscopic two-segment colectomy.
CASE PRESENTATION
A 70-year-old man who was positive for a blood stool test visited our hospital. Colonoscopy, computed tomography (CT) and barium enema indicated quadruple concurrent locally advanced cancers. The first tumor, with observed lumen stenosis, was located in the ascending colon; the second tumor was located in the descending colon and the third and fourth tumors were located in the sigmoid colon (Fig. 1). CT revealed marked intestinal wall thickness in the ascending, descending and sigmoid colon (Fig. 2). Preoperative precise simulation using 3D angiography was performed to determine adequate lymph node dissection along the arteries feeding the tumors and appropriate resection to avoid anastomotic leakages.
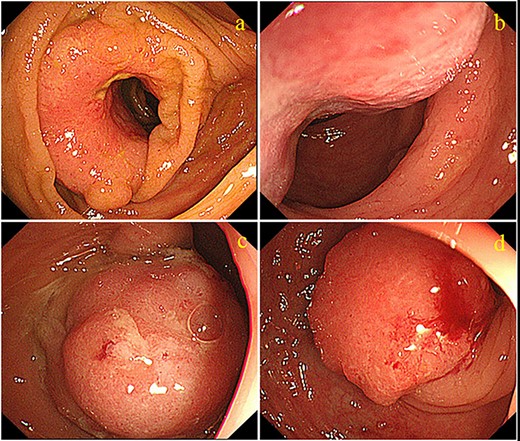
Colonoscopy images showing four tumors. (a) One cauliflower-like tumor with lumen stenosis is located in the ascending colon. (b) Another cauliflower-like tumor is located in the descending colon. The third (c) and fourth (d) tumors are located in the sigmoid colon.
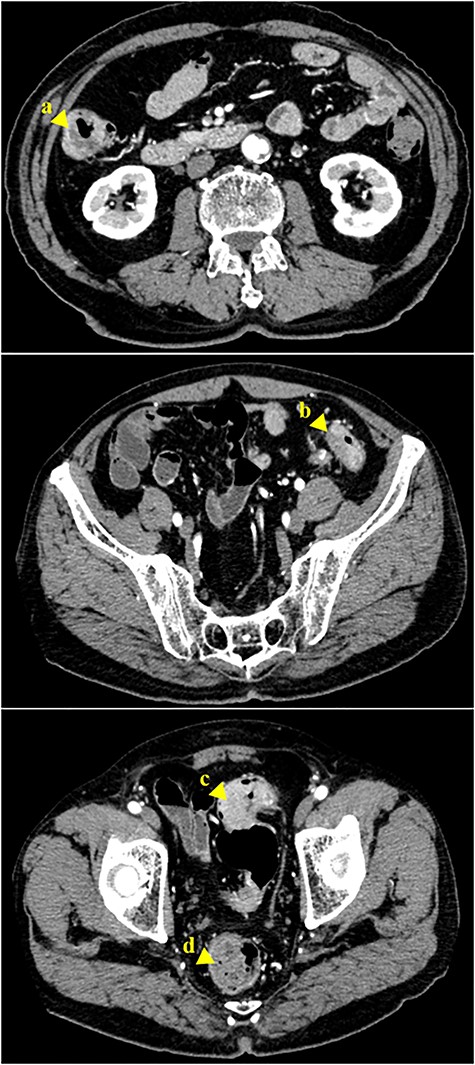
Abdominal CT scan revealing a tumor of the ascending colon (a, arrowhead). A tumor in the descending colon (b, arrowhead), and two tumors in the sigmoid colon are also visible (c, d, arrowhead)
We planned the appropriate placement of trocars as shown in Figure 3, because we wanted to create a single mini-laparotomy for specimen retrieval and extracorporeal reconstruction after lymph node dissection and mobilization of the colon.
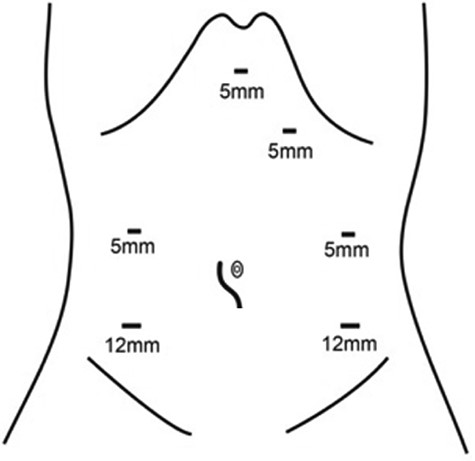
Placement of trocars and mini-incision in the present case
During the operation, laparoscopic exploration confirmed the presence of known four tumors with no invasion of the serosa. Subsequently, a right hemicolectomy and sigmoid colectomy were performed laparoscopically. The right half of the colon was separated, and a side-to-side anastomosis between the jejunum and transverse colon was performed, followed by the sigmoid colon, and a colorectal anastomosis between the descending colon and rectum was performed. The resected tissue specimens revealed four tumors (Fig. 4). Histological examination showed that the first tumor in the ascending colon, the second tumor in the descending colon and the third tumor in the sigmoid colon had invaded up to the subserosa, whereas the fourth tumor in the sigmoid colon had invaded up to the muscularis propria (Fig. 5).
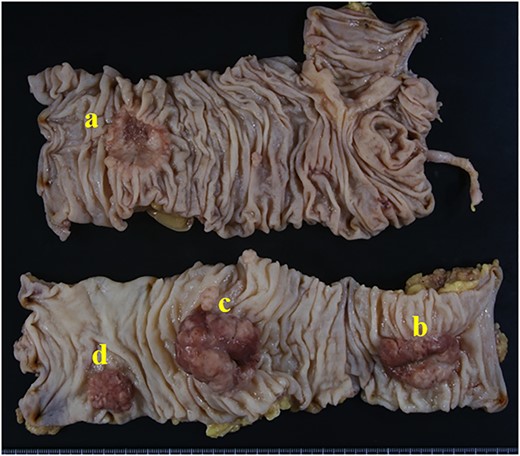
The surgical specimens of the ascending colon cancer (a), descending colon cancer (b) and the two sigmoid colon cancers (c and d).
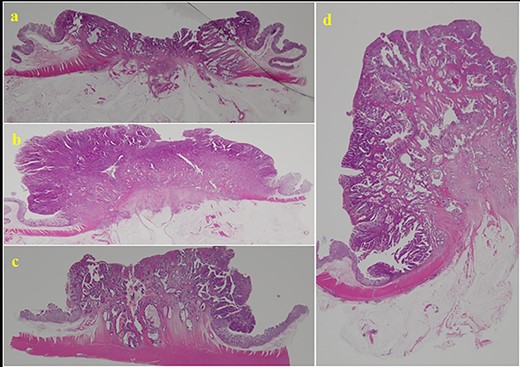
Histopathological examination of the tissue specimens revealed four tumors showing cancerous cells arranged in a tubular pattern.
According to the American Joint Committee on Cancer/Tumor-Node-Metastasis Staging System, the p-stage was IIIa, T3N1M0. The patient was discharged 15 days after surgery. For adjuvant chemotherapy, the patient chose to take an oral fluoropyrimidine agent for 6 months. Fortunately, there have been no signs of metastasis or recurrence after the operation at 64 months of follow-up.
DISCUSSION
We reported a rare case of quadruple SCRCs. All four tumors were removed curatively by laparoscopic surgery with D3 lymph node dissection. We planned a strategy for quadruple SCRCs based on preserving the remnant large intestine and sufficient D3 lymph node dissection through a laparoscopic approach. We believe that laparoscopic surgery can be a safe even for quadruple SCRCs. This is the first case report of laparoscopic surgery with D3 lymph node dissection for quadruple advanced SCRCs.
The incidence of malignant SCRC with four or five synchronous lesions is extremely rare, with a rate of 0.19% being reported [7]. This is a quite rare case of quadruple synchronous advanced cancer arising from the ascending, descending and the sigmoid colon. It was reported that SCRCs often occur in the same or adjacent segment of the large intestine and that other smaller colorectal cancers in the patients with SCRCs were usually smaller and of lower pathological grade and T staging than the index cancer [8]. However, all of the SCRCs in our patient had the same histological grade and T staging (p-stage IIIa), with the tumor locations being in the ascending, descending and sigmoid colon.
Surgical management of SCRCs needs to be tailored to the individual based on tumor location, invasion status and the patient’s health condition. Some studies have suggested total or subtotal colectomy to remove any potential existing synchronous tumors or polyps that have not been detected [9]. However, other studies recommend a more conservative surgical approach [10]. It is thought that the removal of the entire colon will prevent the development of metachronous tumors, and a previous study indicated that subtotal colectomy may increase defecation frequency as the normal colon cannot be preserved [8]. We successfully performed laparoscopic surgery combining two-segment resection of a right hemicolectomy and sigmoid colectomy with no intra- or postoperative adverse events. In our patient, we tried preserving as much colon as possible considering the patient’s quality of life after surgery in addition to performing sufficient D3 dissection. Of course, the meaning of preserving colon in terms of patient postoperative quality of life needs to be more clearly assessed in future.
We encountered a rare case of advanced quadruple SCRCs for which we achieved a curative resection that required two anastomoses through a laparoscopic approach. We suggest that laparoscopic surgery that requires multiple anastomoses for advanced SCRCs can be a safe procedure even if the number of colorectal cancers is multiple.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
None.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}