





Abstract
As the desire for an intersex phenotypic condition increases, surgeons need to become aware of the surgical possibilities there are realistic expectations and a sound mind. A 43-year-old married cis-gender female, on testosterone desired conversion of her enlarged clitoris into a micropenis or metoidioplasty without scrotoplasty or urethral lengthening to increase the size and accentuate her orgasmic response. Following clearance by mental health, a diamond perineoplasty and metoidioplasty using her labia minora was performed. At 1 year her Arizona Sexual Experience Scale increased and she was happy with the operation. Creation of a micropenis, in a cis-gender patient for an intersex state and heightened orgasmic response is surgically feasible.
INTRODUCTION
‘Intersex’ is a general term used for a variety of conditions in which a person is born with a reproductive or sexual anatomy that does not seem to fit the typical definitions of female or male.
Ancient Jewish commentary on the first book of the Bible, suggests that God created an androgyne in his own image and only later divided it into male and female [1]. In this view, only intersexual people are created in the image of God. This ideology has led to some individuals desiring an intersex condition. Surgery for an intersex condition may be difficult to achieve due to lack of awareness and experience, but it may be performed. There are no defined guidelines for this phenotypic transition like there are for gender transition [2]; however, a mental health evaluation to document mental stability and proper informed consent is advised as these are not routine procedures.
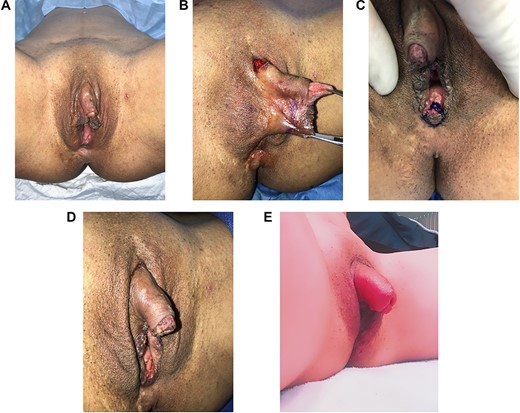
(A) Patient prior to surgery. Note hypertrophic clitoris and labia minora; (B) intraoperative photo of incision used for clitoral suspensory ligament release, and labia minora reduction prior to creation of micropenis; (C) diamond perineoplasty after creation of micropenis for narrowing of vaginal canal; (D) immediate postoperative photo after creation of micropenis, clitoral suspensory ligament release, labia minora reduction and perineoplasty; (E) 1-year postoperative and following use of clitoral suction device for enlargement of clitoris. Improvement in ASEX score and having penetrative vaginal intercourse.
CASE REPORT
We present a case of a 43-year-old G2P2, married, cis-gender female who presented on testosterone orally and topical dihydrotestosterone to her clitoris to increase in size. The patient did not suffer from gender dysphoria and had a healthy social and sexual relationship with her husband. The patient was cleared by our center’s psychologist and deemed mentally competent to make her decisions regarding surgery and consent. She also completed the Arizona Sexual Experiences Scale (ASEX) for an objective evaluation following surgery [3]. The patient desired conversion of her enlarged clitoris into a micropenis or metoidioplasty without scrotoplasty or urethral lengthening, in addition to vaginal tightening at the introitus for self-reported vaginal laxity. Her desire was to have mobile skin completely around her enlarged clitoris as a penis would. Upon physical examination it was noted that her clitoris and labia minora tissues were hypertrophic and a relaxed vagina existed whereby four digits readily passed in the vaginal canal (Fig. 1A).
After informed consent was obtained, a general anesthetic was used and the patient was placed in the lithotomy position. The markings were performed and local anesthetic with epinephrine was used. The clitoral suspensory ligament at the apex of the clitoral hood was dissected with loupe magnification avoiding injury to the two clitoral nerves and this was released allowing lengthening of the clitoris. An inferior wedge resection of the labia minora with circumferential wrap of the clitoral body for creation of a micropenis (Fig. 1B) was then performed and a diamond perineoplasty to narrow the vaginal introitus so that only two digits would be readily inserted into the vaginal canal. (Fig. 1C and D).
The patient was discharged following surgery and not allowed to resume vaginal intercourse for 2 months. She was allowed to exercise at 6 weeks. She had no complications and her ASEX Score after surgery was 5 at 5 months.
At 1 year she had resumed penetrative vaginal intercourse with orgasm at 3 months, and had improved erogenous sensation in her now micropenis, in addition to improvement in her ASEX score to 5 when previously it was 12. (Average score for adults (patients and controls) without clinical sexual dysfunction is 14 in women and 10 in men). The patient also began using a clitoris suction device after the 1 year to further enlarge its size (Fig. 1E).
DISCUSSION
Creation of a micropenis, in a cis-gender person for the purposes of an intersex state or phenotype and heightened orgasmic response has not been previously published. It may be surgically feasible if the patient has been properly evaluated and deemed competent to make a properly informed consent decision. An intersex condition is not related to one’s identity. The surgical transformation to this condition may be reversible if desired and therefore advantageous in cases of regret. In this cis-gender heterosexual patient, she presented with her husband, on anabolic steroids, and with pre-existing clitoral hypertrophy. Her desire was to have her enlarged clitoris to be converted to a micropenis, which she believed would lead to a heightened sexual response upon stimulation, and a more narrow vaginal canal primarily at the introitus to treat her self-reported laxity. Although an unusual request for elective surgery, the patient was of sound mind and this reversible surgery could be performed to meet the patient’s expectations. We feel this is an advancement of not only plastic surgery due to new potential treatment of those individuals who desire an intersex condition but also potentially mental health treatmemt if patient dysphoria exists with this desire of an intersex condition.

{kind=link}