





Abstract
Sinking skin flap syndrome is a rare syndrome leading to increased intracranial pressure, known to neurosurgeons, yet uncommon and hardly ever reported in trauma patients. In a hospitalized trauma patient with declining neurological status, rarely do we encounter further deterioration by elevating the patients’ head, diuresis and hyperventilation. However, after craniectomy for trauma, a partially boneless cranium may be compressed by the higher atmospheric pressure, that intracranial pressure rises to dangerous levels. For such cases, paradoxical supportive management with intravenous fluid infusion, and reverse Trendelenburg positioning, is used to counteract the higher atmospheric pressure, as a bridge to definitive treatment with cranioplasty. These steps constitute an urgent and easily applied intervention to reduce further neurological deterioration, of which every trauma healthcare provider should be aware.
INTRODUCTION
In the acute trauma setting, hyperosmotic intravenous fluid, head elevation and hyperventilation are the bridging medical options for severe traumatic brain injury prior to decompressive cranial operative intervention in a patient with sinking skin flap syndrome (SSFS), a syndrome characterized by increased intracranial pressure due to external atmospheric pressure, following a craniectomy. Rarely do we encounter deterioration of the neurological exam that is worsened by interventions that are meant to decrease the intracranial pressure (ICP), such as the ones mentioned above.
High clinical suspicion for SSFS during hospitalization helps prevent and mitigate the damage caused by a pressure shift from the higher atmospheric pressure into the cranial space as the initial treatment requires increasing the intracranial pressure.
CASE REPORT
A 59-year-old male was found in the street with a head laceration. He was brought to the trauma bay as a pedestrian struck trauma patient with a prehospital GCS of 3. On arrival, his GCS was 11 (E3, V2, M6). An expanding neck hematoma was seen on exam. CT scan revealed scattered bilateral frontal contusions with hemorrhage in right basal ganglia, small bilateral acute SDH without significant mass effect, minimally displaced right temporal/occipital skull fracture and right-sided rib fractures 1–7 (flail chest) with hemopneumothorax (Fig. 1).
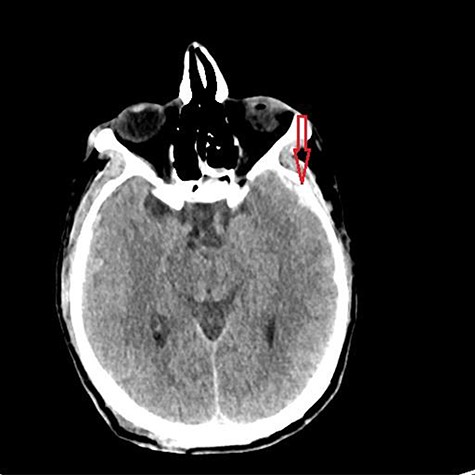
Initial CT head.
He was paralyzed, intubated and taken emergently to the OR due to nonresponsive hypovolemic shock. A right frontal ICP monitor was placed in the operating room while he was undergoing an emergency thoracotomy. Intraoperative ICP was in the 40s, and thus the patient was taken directly from the operating room to CT scan which showed enlargement of bilateral contusions, left greater than right, for which he was taken emergently to the operating room for a left hemicraniectomy (Figs 2 and 3).
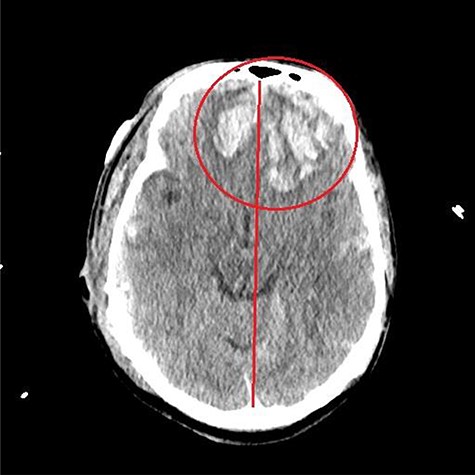
CT head post thoracotomy with expansion of contusion with shift.
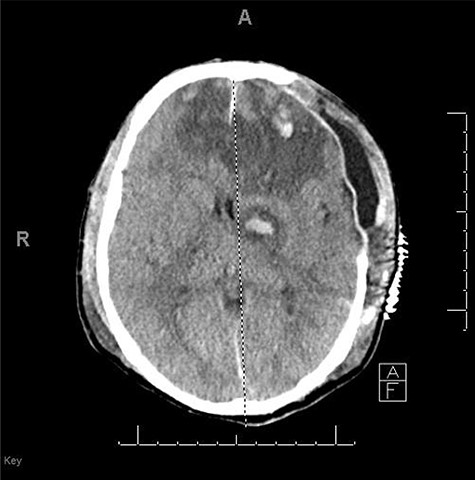
CT head POD3 from craniectomy.
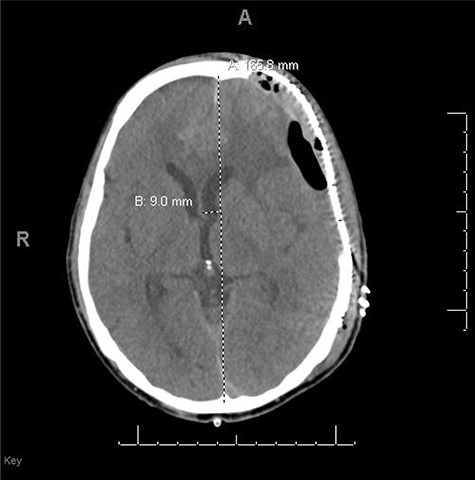
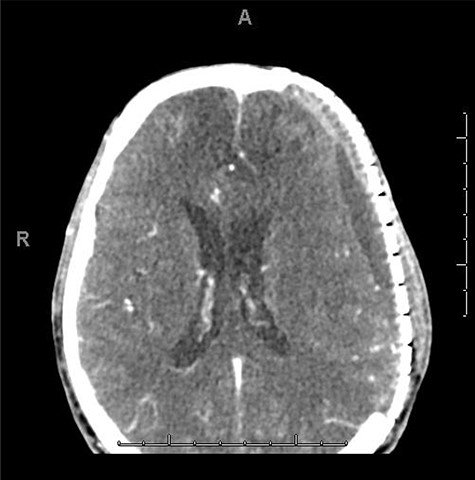
He had a significant recovery, to the point where he was awake with mild right paresis. He was following commands briskly but remained nonverbal. On hospital day 26, he developed neurological deterioration with decreased mental status and worsening right hemiparesis. Clinical examination noted pronounced new indentation of his hemicraniectomy flap site. CT head showed a rightward shift away from the craniectomy site and impending herniation (Fig. 4).

CT head POD26 from craniectomy demonstrating findings consistent with SSFS.
He was positioned in Trendelenburg position and infused with intravenous fluids with some improvement in his symptoms. Based on his clinical and radiographic picture, SSFS was suspected. He was taken to the operating room for an emergency left cranioplasty, with a preformed fronto-temporo-parietal titanium mesh.
He did well after surgery with improvement in his neurological status and a postoperative CT scan showing re-expansion of the brain with a left-sided hygroma underneath the cranioplasty (Fig. 5). He continued to improve neurologically to the point where he was awake, nonverbal, but able to follow commands bilaterally. He was discharged to rehabilitation and was seen in the office with a CT scan of the head a month later showing improvement in the left hygroma (Fig. 6). He was verbal and, although with some cognitive delay, had no focal deficits on physical exam.
s/p cranioplasty.
POD15 from cranioplasty.
DISCUSSION
SSFS, also known as ‘syndrome of the trephined’, was first described in 1939 [1]. Almost a century later, only a few case reports were published by trauma centers. The increased incidence of traumatic brain injury and craniectomies in the USA [2] could potentially lead to an increased number of patients at risk of developing SSFS. Trauma residents, physician assistants and attendings should be aware of this syndrome and its presentation. SSFS can present with sudden or progressive symptoms of weakness, lethargy, vertigo, cognitive impairment, headaches or sudden acute neurologic deficits that resolve with temporary measures such as placing the patient in Trendelenburg position and infusing intravenous fluids [3]. SSFS can occur within a few days up to a year after injury [4].
The pathophysiology of SSFS has been hypothesized to be caused by the direct transmission of atmospheric pressure, which is high relative to ICP, directly onto brain tissue. This effect is worsened in the setting of a decreased ICP during the course of healing as mass effect and swelling diminished. As such, loss of the rigid brain encasement resulting from large craniectomies is an important factor [5].
The definitive treatment of this condition is by the closure of the cranial defect with mesh or bone replacement. Patients have a complete recovery from all symptoms following cranioplasty, with partial recovery as the exception. Recovery is described to be typically between 24 hours and 2 weeks. However, late recovery over several months has also been described [3, 6].
Healthcare providers should be aware of SSFS and should have high clinical suspicion when trauma patients with craniectomies develop neurological changes to avoid unnecessary testing and to mitigate brain injury. Daily, well-documented physical exams are crucial for tracking the development of a sunken flap, but not all those who have a concave flap will develop symptoms. In a review of 83 patients with SSFS, all those patients had a depressed skin flap at the time of diagnosis. Some of those patients worked up solely because of the depressed skin flap, without a change in the patients’ clinical status, and were diagnosed after imaging. Other patients developed symptoms, including motor, cognitive and or sensory along with the depressed skin flap, that lead to the diagnosis [4].
In conclusion, whether SSFS is present or not, urgent intervention is generally needed for acute deterioration of mental status in the trauma population. Familiarity with SSFS and its acute management will allow it to be ruled in or out, and further management can be performed according to the appropriate algorithm. In the case of SSFS, urgent cranioplasty is the definitive method of treatment.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}