





Abstract
Metastatic salivary gland tumors are rare clinical entities of the head and neck. Parotid gland carcinoma with distant metastases heralds a poor prognosis with a median survival of 4.3–7.3 months. The lungs, long bones, liver and brain are the most common sites of metastasis for parotid gland cancer, along with a few reported cases describing metastasis to the ileum, spleen and iliac crest. We present the first case to our knowledge of parotid adenocarcinoma metastasis to the breast.
INTRODUCTION
The World Health Organization describes 11 benign and 22 malignant subtypes of epithelial salivary gland tumors [1], yet salivary gland tumors account for <2% of head and neck neoplasms. Primary salivary gland malignancies represent <5% of all head and neck cancers [2]. Furthermore, metastatic salivary gland tumors are rare clinical findings as only 20% of patients with parotid gland malignancy develop metastatic disease. The presence of distant metastases heralds a poor prognosis with median survival of 4.3–7.3 months [3]. The common parotid malignancy metastatic sites include lungs, bones, liver and central nervous system [4]; however, a few reports describe parotid cancer metastasis to the ileum, spleen and iliac crest [3,5–7]. We report a case of parotid gland adenocarcinoma with metastasis to the breast, which to our knowledge has never been described in the literature.
CASE REPORT
A 58-year-old female with history of cervical cancer presented with 2-week history of a palpable left upper outer quadrant breast mass. She denied mastodynia, nipple discharge or skin retraction. She underwent a left radical parotidectomy for pT4a N0 parotid adenocarcinoma 3 months prior and was undergoing adjuvant radiation for positive margins (60 Gy over 30 fractions with 6 Gy boost to select areas). She was an active 20 pack-year smoker. Her mother and paternal aunt had reported history of breast cancer.
Physical examination yielded a 2-cm well-circumscribed, mobile, non-fixed, palpable mass in the upper outer quadrant of the left breast. She had no axillary lymphadenopathy, nipple retraction, excoriation, drainage or radiation-induced skin changes. Mammography and ultrasound of the breast mass demonstrated a 1.3 × 1.2 × 1.3-cm echogenic mass with irregular margins and posterior enhancement (Fig. 1). Core needle biopsy demonstrated adenocarcinoma that was morphologically identical to the patient’s known parotid malignancy.
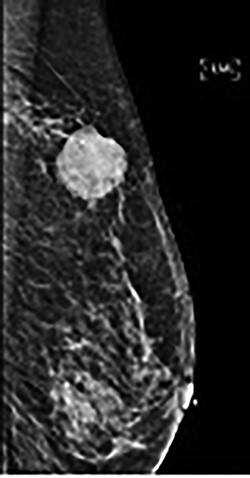
Mammography of palpable mass.
She underwent surgical excision of the breast mass. Final pathology confirmed poorly differentiated carcinoma morphologically identical to her known parotid adenocarcinoma (Fig. 2).
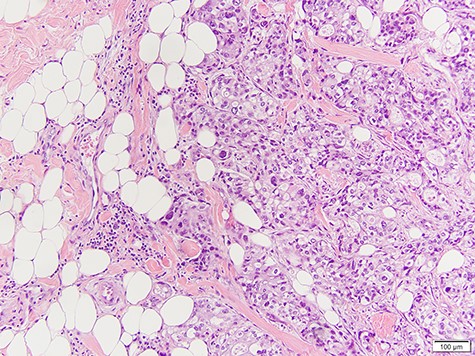
Infiltration of high-grade poorly differentiated malignant cells from breast biopsy.
Two months after metastasectomy, she moved closer to family. Care was transitioned to an oncologist in her new location and she had no further follow-up with our institution. Per communication with her new provider, she developed widespread metastasis in her bones, brain, liver and bilateral adrenal glands 3 months later. She was enrolled in hospice care.
DISCUSSION
Malignant parotid tumors typically spread via lymphatics to cervical lymph nodes with rare hematogenous spread to distant sites [8]. When distant metastases are identified, the lungs, bones, liver and brain are the most frequently involved sites [4]. This case of breast metastasis appears to be the first of its kind to be reported. A search of the PubMed database over a 36-year period (1982–2018) yielded no reported cases. There was one report of parotid carcinoma ex pleomorphic adenoma metastasis to the ileum [3] and another report with metastasis to the spleen [5] as well as two reports of parotid acinic cell carcinoma with iliac crest metastasis [6–7].
Due to the rarity of this malignancy, standardization of systemic therapy for salivary gland cancers has posed a long-standing problem. Treatment options for metastatic adenocarcinoma of the parotid gland are based heavily upon clinical experience and retrospective studies. Surgical resection of the parotid gland with metastasectomy followed by adjuvant radiotherapy is a current appropriate treatment strategy [9]. The role of chemotherapy for treatment of salivary gland cancer remains controversial. While chemotherapy alone does not offer significant survival benefit, literature has shown chemo-radiotherapy regimens that improve radiotherapy efficacy via radiosensitization while providing adjuvant systemic therapy against distant micrometastasis [10].
Due to low incidence, reported epidemiological knowledge of malignant neoplasms of the parotid gland is scarce [9]. Though rare, they still constitute a serious health burden in the general population due to poor prognosis and potential for distant metastasis [3–7]. Long-term follow-up and high clinical suspicion is crucial for early diagnosis of salivary gland cancer metastasis. Through early detection and treatment, local or systemic tumor recurrence may be prevented [9]. Further research is warranted to assess the impact of early detection of parotid metastasis on survival and recurrence.
CONCLUSION
This case of metastatic parotid adenocarcinoma presenting as new breast mass enhances the literature describing a novel clinical presentation of this disease and highlights the importance of maintaining a broad differential diagnosis when evaluating breast lesions. This also emphasizes necessity for lifelong follow-up and clinical assessment in patients with malignant salivary gland tumors. We report a novel case of parotid adenocarcinoma metastasizing to the breast.
CONFLICTS OF INTEREST STATEMENT
The authors state they have no conflicts of interest for this report.

{kind=link}
{kind=link}